- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Learn Basic Laparoscopic Surgery, the components of a laparoscopic surgical setup, optimal positioning and ergonomics in laparoscopic surgery, and much more. Check out the full course for free here: https://www.incision.care/free-trial
What is Laparoscopic Surgery:
Laparoscopic surgery describes procedures performed using one or multiple small incisions in the abdominal wall in contrast to the larger, normally singular incision of laparotomy. The technique is based around principles of minimally invasive surgery (or minimal access surgery): a large group of modern surgical procedures carried out by entering the body with the smallest possible damage to tissues. In abdominopelvic surgery, minimally invasive surgery is generally treated as synonymous with laparoscopic surgery as are procedures not technically within the peritoneal cavity, such as totally extraperitoneal hernia repair, or extending beyond the abdomen, such as thoraco-laparoscopic esophagectomy. The term laparoscopy is sometimes used interchangeably, although this is often reserved to describe a visual examination of the peritoneal cavity or the purely scopic component of a laparoscopic procedure. The colloquial keyhole surgery is common in non-medical usage.
Surgical Objective of Laparoscopic Surgery:
The objective of a laparoscopic approach is to minimize surgical trauma when operating on abdominal or pelvic structures. When correctly indicated and performed, this can result in smaller scars, reduced postoperative morbidity, shorter inpatient durations, and a faster return to normal activity. For a number of abdominopelvic procedures, a laparoscopic approach is now generally considered to be the gold-standard treatment option.
Definitions
Developments of Laparoscopic Surgery:
Following a number of smaller-scale applications of minimally invasive techniques to abdominopelvic surgery, laparoscopic surgery became a major part of general surgical practice with the introduction of laparoscopic cholecystectomy in the 1980s and the subsequent pioneering of endoscopic camera technology. This led to the widespread adoption of the technique by the early- to mid-1990s. The portfolio of procedures that can be performed laparoscopically has rapidly expanded with improvements in instruments, imaging, techniques and training — forming a central component of modern surgical practice and cross-specialty curricula [2]. Techniques such as laparoscopically assisted surgery and hand-assisted laparoscopic surgery have allowed the application of laparoscopic techniques to a greater variety of pathology. Single-incision laparoscopic surgery, natural orifice transluminal endoscopic surgery, and minilaparoscopy-assisted natural orifice surgery continue to push forward the applications of minimally invasive abdominopelvic techniques; however, the widespread practice and specific indications for these remain to be fully established. More recently, robotic surgery has been able to build on laparoscopic principles through developments in visualization, ergonomics, and instrumentation.
This Basic Laparoscopic Surgery Course Will Teach You:
- Abdominal access techniques and the different ways of establishing a pneumoperitoneum
- Principles of port placement and organization of the operative field
- Key elements of laparoscopic suturing, basic knotting and clip application
Specific attention is paid to the following hazards you may encounter:
- Fire hazard and thermal injury
- Lens fogging
- Contamination of insufflation system
- Complications from trocar introduction
- Limitations of Veress needle technique
- Limitations of open introduction technique
- Complications of the pneumoperitoneum
- Gas embolism
- Mirroring and scaling of instrument movements
- Firing clip applier without a loaded clip
The following tips are designed to improve your understanding and performance:
- Anatomy of a laparoscope
- Checking for optic fiber damage
- "White balance" of camera
- Checking integrity of electrosurgical insulation
- Access at Palmer's point
- Lifting abdominal wall before introduction
- Confirming position of Veress needle
- Umbilical anatomy
- Identification of inferior epigastric vessels under direct vision
- Translumination of superficial epigastric vessels
- Selection of trocar size
- Aiming of trocar
- Working angles in laparoscopic surgery
- Choice of suture material
- Instruments for suturing
- Optimal ergonomics for suturing
- Extracorporeal needle positioning
- Optimal suture lengths
- "Backloading" needle
- Intracorporeal needle positioning
- Hand movements when suturing
- Optimal positioning of scissors
- Extracorporeal knot tying
- Visualization of clip applier around target structure
- Common clip configurations
This video illustrates several forms of catatonia including waxy flexibility, forced grasping, opposition, negativism and aversion.

Join Dr. Parsia Vagefi, Chief of Surgical Transplantation and Dr. Steven Hanish, Surgical Director of Liver Transplantation, as they grant unprecedented access to the OR while performing a #Liver #Transplant #Surgery.
To find out more about UT Southwestern's transplant programs visit:
https://www.utswmed.org/transplant

Brain tumor survivor Robert Alvarez and neurosurgeon Sujit Prabhu, M.D., explain why and how Robert played the guitar during his surgery for a grade II astrocytoma. It was the first time a brain tumor patient played a musical instrument during an awake craniotomy at MD Anderson.
Read Robert Alvarez's story: https://www.mdanderson.org/pub....lications/cancerwise
Learn about awake craniotomy for brain tumors: https://www.mdanderson.org/pub....lications/cancerwise
Request an appointment at MD Anderson by calling 1-877-632-6789 or online at: https://my.mdanderson.org/Requ....estAppointment?cmpid

For more than 25 years, The Children's Hospital of Philadelphia — the first Level 1 Pediatric Trauma Center in Pennsylvania — has provided unparalleled medical and surgical care for all injured children, including those with the most severe injuries.
Learn what makes the Trauma Center at CHOP a Level 1 Pediatric Trauma Center, and how our work toward trauma prevention, research advances and overall trauma awareness provides hope for reduced injuries in the future.
Learn more about the Trauma Center at CHOP: http://www.chop.edu/trauma.

Once the diagnosis of a splenic abscess has been made, the patient must be admitted to the hospital and treated. Treatment depends on the patient's overall condition, comorbidities, and primary disorder (if any), as well as the size and topography of the abscess
Venous cutdown is an emergency procedure in which the vein is exposed surgically and then a cannula is inserted into the vein under direct vision. It is used to get vascular access in trauma and hypovolemic shock patients when peripheral cannulation is difficult or impossible

all yo need to know about the female orgasm
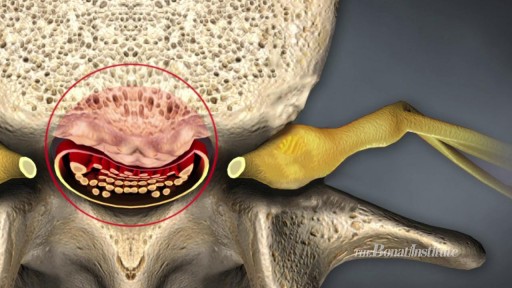
Watch Spinal Stenosis Videos Spinal stenosis occurs when the spinal cord in the neck (cervical spine) or the spinal nerve roots in the lower back (lumbar spine) are compressed. Symptoms of lumbar stenosis often include leg pain (sciatica) and leg tingling, weakness, or numbness. Arm pain is a typical symptom of cervical spinal stenosis. For cervical spinal stenosis with myelopathy, difficulty with coordination often occurs. Stenosis treatment may include non-surgical options (exercise, anti-inflammatory medication, epidural injections, and activity modification) or back surgery.

How to push a baby out video how to prevent tearing during labor and delivery

Doctor Ricky Brown reacts to this surgery simulation of an inguinal hernia repair where they repair the hernia sack and create a mesh for the organ to comfortably rest on.
3D Animation powered by:
3DMedWorld - 3dmedworld.com
#shorts #doctor #education #surgery #medical

Give away to who ever that will correctly mention the sample specimen used to make this video? (Be specific)
DROP ON THE COMMENT BOX

A grand mal seizure causes a loss of consciousness and violent muscle contractions. It's the type of seizure most people picture when they think about seizures. A grand mal seizure — also known as a generalized tonic-clonic seizure — is caused by abnormal electrical activity throughout the brain. Usually, a grand mal seizure is caused by epilepsy. But sometimes, this type of seizure can be triggered by other health problems, such as extremely low blood sugar, a high fever or a stroke. Many people who have a grand mal seizure never have another one and don't need treatment. But someone who has recurrent seizures may need treatment with daily anti-seizure medications to control and prevent future grand mal seizures

Common Benign Pain Syndromes--Symptoms and Etiology:
1. Non-specific musculoskeletal pain: This is the most common cause of back pain. Patients present with lumbar area pain that does not radiate, is worse with activity, and improves with rest. There may or may not be a clear history of antecedent over use or increased activity. The pain is presumably caused by irritation of the paraspinal muscles, ligaments or vertebral body articulations. However, a precise etiology is difficulty to identify.
2. Radicular Symptoms: Often referred to as "sciatica," this is a pain syndrome caused by irritation of one of the nerve roots as it exits the spinal column. The root can become inflamed as a result of a compromised neuroforamina (e.g. bony osteophyte that limits size of the opening) or a herniated disc (the fibrosis tears, allowing the propulsus to squeeze out and push on the adjacent root). Sometimes, it's not precisely clear what has lead to the irritation. In any case, patient's report a burning/electric shock type pain that starts in the low back, traveling down the buttocks and along the back of the leg, radiating below the knee. The most commonly affected nerve roots are L5 and S1.
3. Spinal Stenosis: Pain starts in the low back and radiates down the buttocks bilaterally, continuing along the backs of both legs. Symptoms are usually worse with walking and improve when the patient bends forward. Patient's may describe that they relieve symptoms by leaning forward on their shopping carts when walking in a super market. This is caused by spinal stenosis, a narrowing of the central canal that holds the spinal cord. The limited amount of space puts pressure on the nerve roots when the patient walks, causing the symptoms (referred to as neurogenic claudication). Spinal stenosis can be congenital or develop over years as a result of djd of the spine. As opposed to true claudication (pain in calfs/lower legs due to arterial insufficiency), pain resolves very quickly when person stops walking and assumes upright position. Also, peripheral pulses should be normal.
4. Mixed symptoms: In some patients, more then one process may co-exist, causing elements of more then one symptom syndrome to co-exist.

Oral sex is a commonly performed act of foreplay involving the kissing or licking of the genital area to pleasure a partner. However, it is sometimes stated that the act alone can increase the risk of throat cancer. Is this really the case?
ost of us come across this particular sign quite often. Of course, you can just jump to the numerous investigations and one after another, rule out the possible causes, finally getting to the diagnosis. For me, that’s no fun at all. Although I still don’t know whether I am going to become a surgeon or not (embarassing for me, since I’m going to be done with med-school this year), its pretty fascinating. If I were to work in a country whether investigations aren’t that expensive, I would definitely just perform a small examination and take a short history, sending off my patient to get a myriad of investigations, reporting to me after a while, with the diagnosis in his reports.

Elbow Exam - Orthopaedic OSCE - Clinical Skills - Dr Gill
The elbow examination is a core skill - in this video, we demonstrate how to perform an elbow EXAM for an Orthopaedic Clinical Skills OSCE, which should be one of the more accessible examination stations for medical students.
For a passing grade in your Clinical Skills OSCE, an elbow assessment should follow the LOOK, FEEL, MOVE approach
Initially looking for erythema, scars, swelling and position
Palpating the elbow - specifically the olecranon, medial and lateral epicondyles, and radial head for heat, oedema and crepitus
Finally assess range of movement with flexion and extension at the elbow, before determining for tennis and golfers' elbows
Watch further orthopaedic examinations for your OSCE revision:
The Elbow - Deep Dive
https://youtu.be/SX5buhtCVDw
The Spine Examination:
https://youtu.be/pJxMHa6SCgU
The Knee examination
https://youtu.be/oyKH4EYfJDM
The Hip examination
https://youtu.be/JC9GKq5nSdQ
The GALS examination
https://youtu.be/5qJaf7gW-B0 - Gait, Arms, Legs, Spine - GALS screen
------------
Please note that there is no ABSOLUTE way to perform a clinical examination. Different institutions and even clinicians will have differing degrees of variations - the aim is the effectively identify medically relevant signs.
However during OSCE assessments. Different medical schools, nursing colleges and other health professional courses will have their own preferred approach to a clinical assessment - you should concentrate on THEIR marks schemes for your assessments.
The examination demonstrated here is derived from Macleods Clinical Examination - a recognised standard textbook for clinical skills.
Some people viewing this medical examination video may experience an ASMR effect
#clinicalskills #Elbow #DrGill

Adenocarcinoma of the Transverse Colon taken by Dr. Julio Murra Saca This is the case of a 42 year-old male, with no significant past medical history presented with abdominal pain and no weight loss was reported. Adenocarcinoma of the colon is a primary cause of mortality and
morbidity in North America and Western Europe. Colonic cancers are the most common GI carcinomas and have the best prognosis. The 5-year survival rate is approximately 50%.
Survival rates may be improved by screening and removal of adenomatous polyps. Almost all colonic cancers are primary adenocarcinomas.
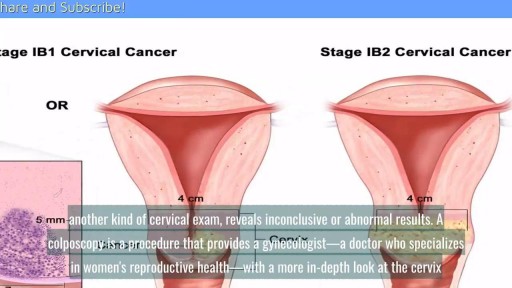
A cervical biopsy is a procedure that is sometimes done on women during an exam called a colposcopy to remove cervical tissue for examination. It is also called a punch biopsy. It is usually performed when a Pap smear result is either inconclusive or abnormal and a doctor wants to screen further for any cervical dysplasia or cervical cancer.

Twin Childbirth Video
