- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

If you’re wondering ‘what’s the cause of my knee pain?’ or ‘what kind of knee pain do I have?’ the position of your knee pain can often tell you what type of knee pain you have.
You confirm this if you know the common symptoms an aggravations for each type of knee problem. So if you want to know ‘why my knee hurts’... here’s a quick look at the most common type of knee problems...
Patellofemoral Pain Syndrome (Or Runner’s Knee) (Old Name: Chondromalacia Patellae)
Infrapatellar Fat Pad Syndrome (Hoffa's Syndrome)
Patella Tendonitis (Jumper’s Knee)
Prepatellar Bursitis
Osgood-Schlatter Disease
Meniscus Tear
Medial Collateral Ligament Tear
Osteoarthritic Knee Pain
Pes Anserine Bursitis.
Iliotibial Band Syndrome
Quadriceps Tendinopathy
Popliteus Strain
Baker’s Cyst
ACL Or PCL Tear/Rupture
---------------------------------------
Check out my channel...
https://youtube.com/@BodyFixExercises
OTHER VIDEOS:
How To Fix Pain In The Front Of The Knee… (Runner's Knee) https://youtu.be/g0qmx_0enAA
Knee Strengthening Exercises To Prevent Knee Pain
https://youtu.be/Pk-ae_lyx7M
How To Treat Patellar Tendinopathy (Jumper’s Knee) & Quadriceps Tendinopathy
https://youtu.be/MkPwsb-rQwU
---------------------------------------
#bodyfixexercises #kneepainrelief #kneepain

For more information on peritoneal dialysis: https://www.massgeneralbrigham.....org/en/about/newsro
Why does someone need dialysis? What is peritoneal dialysis? How does it work? John Kevin Tucker, M.D., Nephrologist at Brigham and Women's Hospital and Vice President for Education at Mass General Brigham, discusses peritoneal dialysis and its benefits for people who have lost their kidney function.
Subscribe Link: https://www.youtube.com/channe....l/UCYrLjATd88gPwIKnt
0:00 - Intro
0:24 - Why Do I Need Dialysis?
1:42 - Treatment
2:02 - Why Is It Called Peritoneal Dialysis
2:35 - 2 Forms of Peritoneal Dialysis
3:50 - Continuous Cycling Peritoneal Dialysis
4:38 - Myths
5:55 - Preparing For Peritoneal Dialysis
About Mass General Brigham:
Mass General Brigham combines the strength of two world-class academic medical centers, five nationally ranked specialty hospitals, 11 community hospitals, and dozens of health centers. Our doctors and researchers accelerate medical breakthroughs and drive innovations in patient care. They are leaders in medical education, serving as Harvard Medical School faculty and training the next generation of physicians. Mass General Brigham’s mission is to deliver the best, affordable health care to patients everywhere. Together, we transform the health of our communities and beyond.
#MassGeneralBrigham #Peritoneal #Dialysis
Visit Mass General Brigham: https://www.massgeneralbrigham.org/
Find us on social:
Twitter: https://twitter.com/MassGenBrigham
Instagram: https://www.instagram.com/massgeneralbrigham/
Facebook: https://www.facebook.com/MassGeneralBrigham/
LinkedIn: https://www.linkedin.com/compa....ny/mass-general-brig
Mass General Brigham:
https://www.youtube.com/massgeneralbrigham
Peritoneal Dialysis: At Home Treatment for Kidney Failure | Mass General Brigham
https://youtu.be/of1T6hMEN_Q

http://www.handalplasticsurgery.com/ 561-912-9888
Orbera intragastric balloon for weight loss

Best and 100% Successful Hymen Repair Surgery in Delhi with Latest Ultrafine Hymen repair Technology. 100% successful , Secure and Private. for more information visit: http://www.olmeccosmeticsurgery.com/best-hymenoplasty-surgery-india-delhi/

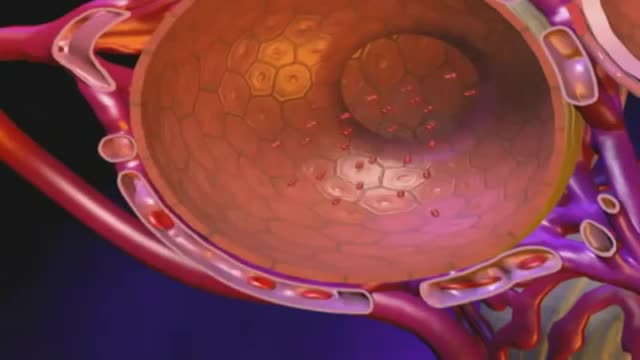
External cephalic version, or version, is a procedure used to turn a fetus from a breech position or side-lying (transverse) position into a head-down (vertex) position before labor begins. When successful, version makes it possible for you to try a vaginal birth.

Our General Surgery team treats hernia patients on a daily basis. In fact, you could consider them to be hernia experts. We sat down with one of those experts, Dr. Heater Dunlap, to talk about the common signs and symptoms of hernias and to answer the question of when to see a doctor.
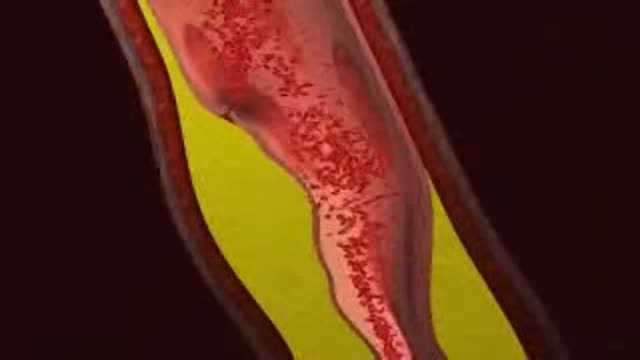
Myocardial infarction (MI), commonly known as a heart attack, is defined pathologically as the irreversible death of myocardial cells caused by ischemia. Clinically, MI is a syndrome that can be recognized by a set of symptoms, chest pain being the hallmark of these symptoms in most cases, supported by biochemical laboratory changes, electrocardiographic (ECG) changes, or findings on imaging modalities able to detect myocardial injury and necrosis. According to the third universal definition of MI, implemented by a joint task force from the European Society of Cardiology (ESC), American College of Cardiology (ACC) Foundation, American Heart Association (AHA), and the World Heart Federation (WHF), MI is diagnosed when either of the following two criteria are met

Originally broadcast November 21, 2014.
They advertise low, low prices. But does anyone actually pay that rate? Erica Johnson investigates.
More from CBC Marketplace, Canada's top consumer affairs show:
Watch episodes online at http://cbc.ca/marketplace
Like us on Facebook: http://facebook.com/cbcmarketplace
Talk to us on Twitter: http://twitter.com/cbcmarketplace
Follow our hosts @cbctom and @cbcerica
Bronchiectasis is an abnormal dilation of the proximal and medium-sized bronchi (>2 mm in diameter) caused by weakening or destruction of the muscular and elastic components of the bronchial walls. Affected areas may show a variety of changes, including transmural inflammation, edema, scarring, and ulceration, among other findings. Distal lung parenchyma may also be damaged secondary to persistent microbial infection and frequent postobstructive pneumonia. Bronchiectasis can be congenital but is most often acquired.[9] Congenital bronchiectasis usually affects infants and children. These cases result from developmental arrest of the bronchial tree. Acquired forms occur in adults and older children and require an infectious insult, impairment of drainage, airway obstruction, and/or a defect in host defense. The tissue is also damaged in part by the host response of neutrophilic proteases, inflammatory cytokines, nitric oxide, and oxygen radicals. This results in damage to the muscular and elastic components of the bronchial wall. Additionally, peribronchial alveolar tissue may be damaged, resulting in diffuse peribronchial fibrosis.[12] The result is abnormal bronchial dilatation with bronchial wall destruction and transmural inflammation. The most important functional finding of altered airway anatomy is severely impaired clearance of secretions from the bronchial tree. Impaired clearance of secretions causes colonization and infection with pathogenic organisms, contributing to the purulent expectoration commonly observed in patients with bronchiectasis. The result is further bronchial damage and a vicious cycle of bronchial damage, bronchial dilation, impaired clearance of secretions, recurrent infection, and more bronchial damage

Outpatient -- or same-day -- knee replacement surgery is more convenient than traditional knee replacement surgery and often can help you recover faster.
Outpatient -- or same-day -- knee replacement surgery is more convenient than traditional knee replacement surgery and often can help you recover faster. At Duke Ambulatory Surgery Center Arringdon, your knee replacement will be followed immediately by physical therapy to get you moving and start your recovery process right away. Our expert joint replacement team ensures your knee replacement surgery is safe and effective so you can return to the comfort of your home as soon as possible.

Doctor Ricky Brown reacts to this surgery simulation of an inguinal hernia repair where they repair the hernia sack and create a mesh for the organ to comfortably rest on.
3D Animation powered by:
3DMedWorld - 3dmedworld.com
#shorts #doctor #education #surgery #medical

This video demonstrates Laparoscopic Cholecystectomy Fully Explained Skin-to-Skin Video with Near Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. A laparoscopic cholecystectomy is a minimally invasive surgical procedure that involves removing the gallbladder. It is typically performed using small incisions in the abdomen, through which a laparoscope (a thin tube with a camera and light) and surgical instruments are inserted. The surgeon uses the laparoscope to visualize the inside of the abdomen and to guide the instruments in removing the gallbladder.
Near-infrared cholangiography is a technique that uses a special camera and fluorescent dye to visualize the bile ducts during surgery. The dye is injected into the cystic duct (the tube that connects the gallbladder to the bile ducts) and the camera detects the fluorescence emitted by the dye, allowing the surgeon to see the bile ducts more clearly.
The combination of laparoscopic cholecystectomy and near-infrared cholangiography has become a standard of care in many hospitals and surgical centers. It allows for a more precise and efficient surgery, reducing the risk of complications such as bile duct injury.
The use of indocyanine green (ICG) with near-infrared imaging during laparoscopic cholecystectomy has several advantages. Here are some of them:
Better visualization of the biliary anatomy: ICG with near-infrared imaging allows for better visualization of the biliary anatomy during surgery. This helps the surgeon identify important structures, such as the cystic duct and the common bile duct, and avoid injuring them.
Reduced risk of bile duct injury: With better visualization of the biliary anatomy, the risk of bile duct injury during surgery is reduced. Bile duct injury is a serious complication that can occur during laparoscopic cholecystectomy and can lead to long-term health problems.
Improved surgical precision: ICG with near-infrared imaging also improves surgical precision. The surgeon can better see the tissues and structures being operated on, which can help reduce the risk of bleeding and other complications.
Shorter operating time: The use of ICG with near-infrared imaging can shorten the operating time for laparoscopic cholecystectomy. This is because the surgeon can more quickly and accurately identify the biliary anatomy, which can help streamline the surgery.
Overall, the use of ICG with near-infrared imaging is a valuable tool in laparoscopic cholecystectomy that can improve surgical outcomes and reduce the risk of complications.
Like any surgical procedure, laparoscopic cholecystectomy (gallbladder removal) has potential complications. Here are some of the most common ones:
Bleeding: Bleeding during or after the surgery is a possible complication of laparoscopic cholecystectomy. Most cases are minor and can be easily controlled, but in rare cases, significant bleeding may require a blood transfusion or even additional surgery.
Infection: Any surgical procedure carries a risk of infection. After laparoscopic cholecystectomy, there is a risk of infection at the site of the incisions or within the abdomen. Symptoms may include fever, pain, redness, or drainage from the incision sites.
Bile leakage: In some cases, a small amount of bile may leak from the bile ducts into the abdominal cavity after gallbladder removal. This can cause abdominal pain, fever, and sometimes requires further surgery or treatment.
Injury to nearby organs: During the surgery, there is a small risk of unintentional injury to nearby organs such as the liver, intestines, or bile ducts. This can cause additional complications and may require further treatment.
Adverse reactions to anesthesia: As with any surgery requiring general anesthesia, there is a small risk of adverse reactions to the anesthesia, such as an allergic reaction, respiratory problems, or heart complications.
Most patients recover without complications following a laparoscopic cholecystectomy, but it is important to discuss any concerns or questions with your surgeon beforehand.
Contact us
World Laparoscopy Hospital
Cyber City, Gurugram, NCR Delhi
INDIA : +919811416838
World Laparoscopy Training Institute
Bld.No: 27, DHCC, Dubai
UAE : +971525857874
World Laparoscopy Training Institute
8320 Inv Dr, Tallahassee, Florida
USA : +1 321 250 7653
Regenerate response

50 Orgasms A Day

Train with some of the region’s very best pediatric general surgeons — in a two-year, pediatric surgical fellowship training program at Nemours/Alfred I. duPont Hospital for Children. Our hospital’s Division of Pediatric Surgery is offering this program in affiliation with Sidney Kimmel Medical College at Thomas Jefferson University .
The goal of the fellowship is to give individuals who have completed an accredited general surgery residency advanced knowledge and training in the management and surgical treatment of newborns, infants and children.
Our Fellowship Program
This fellowship will help you prepare for certification by the American Board of Surgery, and is accredited by the Accreditation Council for Graduate Medical Education (ACGME).
The Pediatric Surgery Fellowship aims to:
train a well-rounded, empathetic, safe pediatric surgeon who is confident managing all aspects of the surgical care of children.
steward our fellow in quality improvement projects and methodology, and provide research opportunities.
provide a rigorous didactic curriculum for our fellow utilizing 360 degree feedback.
cultivate opportunities for our fellow to educate residents and students.
encourage our fellow to collaborate across specialties.
develop our fellow’s presentation skills during M&M conferences and multi-disciplinary educational meetings.
The program features the full participation of all nine of the pediatric surgical division’s full-time faculty members. Each of these physicians will contribute greatly to your education. Your training will include operating room and outpatient clinic experience, as well as bedside evaluation of children. You’ll also play a role in the organization of formal teaching conferences, held weekly. Formal rotations will be spent on Pediatric Urology, PICU and Neonatology during the first 12 months. The last year will be spent entirely on the Pediatric Surgical Service.
The majority of your inpatient consultative time will take place at Nemours/Alfred I. duPont Hospital for Children, a freestanding children’s hospital in Wilmington, Del. The hospital:
is nationally ranked by U.S. News & World Report in eight pediatric specialties
recently opened expansion with 260 beds
performs more than 2,800 inpatient and 9,300 outpatient surgical procedures each year in our operating rooms
has an on-site delivery center for newborns with complex congenital anomalies
receives more than 50,000 annual visits in our Emergency Department (ED)
is accredited by The American College of Surgeons as a Level One Pediatric Trauma Center
is accredited by the Commission on Accreditation of Rehabilitation Facilities (CARF)
Visit https://www.nemours.org/educat....ion/gme/fellowships/ to learn more.
How did Mr Bean get himself into pretending to be a doctor?
Measles is a childhood infection caused by a virus. Once quite common, measles can now almost always be prevented with a vaccine. Signs and symptoms of measles include cough, runny nose, inflamed eyes, sore throat, fever and a red, blotchy skin rash. Also called rubeola, measles can be serious and even fatal for small children. While death rates have been falling worldwide as more children receive the measles vaccine, the disease still kills more than 100,000 people a year, most under the age of 5. As a result of high vaccination rates, measles has not been widespread in the United States for more than a decade. Today, the United States averages about 60 cases of measles a year, and most of them originate outside the country. Symptoms ShareTweet May 24, 2014 References See also Cough Runny nose Vital Vaccinations Advertisement Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission. Advertising & Sponsorship PolicyOpportunities Mayo Clinic Store Check out these best-sellers and special offers on books and newsletters from Mayo Clinic. Mayo Clinic A to Z Health Guide The Essential Guide to Prostate Health Mayo Clinic Guide to Pain Relief The Menopause Solution — NEW! The Mayo Clinic Diet Online

Talley + O'Connor's essential video guide to Abdominal Examination is here! Brush up on your skills and be sure to ace your OSCEs!
Any independent vertical movement of the transducer or the patient will affect the hydrostatic column of this fluid-filled system and thus alter the pressure measurements. At some time before or after PAC insertion, the system must therefore be zeroed to ambient air pressure. The reference point for this is the midpoint of the left atrium (LA), estimated as the fourth intercostal space in the midaxillary line with the patient in the supine position. With the transducer at this height, the membrane is exposed to atmospheric pressure, and the monitor is then adjusted to zero. Calibration Once zeroed, the monitoring system must be calibrated for accuracy. Currently, most monitors perform an automated electronic calibration. Two methods are used to manually calibrate and check the system. If the catheter has not been inserted, the distal tip of the PAC is raised to a specified height above the LA. For example, raising the tip 20 cm above the LA should produce a reading of approximately 15 mm Hg if the system is working properly (1 mm Hg equals 1.36 cm H 2 O). Alternatively, pressure can be applied externally to the transducer and adjusted to a known level using a mercury or aneroid manometer. The monitor then is adjusted to read this pressure, and the system is calibrated. Dynamic tuning Central pressures are dynamic waveforms (ie, they vary from systole to diastole) and thus have a periodic frequency. To monitor these pressures accurately, the system requires an appropriate frequency response. A poorly responsive system produces inaccurate pressure readings, and differentiating waveforms (eg, PA from pulmonary capillary wedge pressure [PCWP]) can become difficult. When signal energy is lost, the pressure waveform is dampened. Common causes of this are air bubbles (which are compressible), long or compliant tubing, vessel wall impingement, intracatheter debris, transducer malfunction, and loose connections in the tubing. A qualitative test of the frequency response is performed by flicking the catheter and observing a brisk high-frequency response in the waveform. After insertion, the system can be checked by using the rapid flush test. When flushed, an appropriately responsive system shows an initial horizontal straight line with a high-pressure reading. Once the flushing is terminated, the pressure drops immediately, which is represented by a vertical line that plunges below the baseline. A brief and well-defined oscillation occurs, followed by return of the PA waveform. A dampened system will not overshoot or oscillate, and causes a delay in returning to the PA waveform.

A Pap smear (Papanicolau smear; also known as the Pap test) is a screening test for cervical cancer. The test itself involves collection of a sample of cells from a woman's cervix (the end of the uterus that extends into the vagina) during a routine pelvic exam

How To Breastfeed - Deep Latch Technique
