- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Shamika Burrage survived a near-fatal car accident two years ago, but not without losing something pretty important: her left ear. Now, thanks to a novel procedure performed at an Army medical center in Texas, Burrage is getting that ear back in a most unusual way. Plastic surgeons harvested cartilage from Burrage's ribs to create a new ear and then grew it under the skin of her forearm. Then the doctors at William Beaumont Army Medical Center in El Paso successfully transplanted the ear from her arm to her head. The technique -- a first time in the Army -- is called prelaminated forearm free flap, said Lt. Col. Owen Johnson III, chief of plastic and reconstructive surgery at William Beaumont Army Medical Center. Some of the big advantages of it is that it reduced the chance of more scarring around Burrage's ear. Also, growing the ear under the skin of her forearm allows new blood vessels to form. "(The ear) will have fresh arteries, fresh veins and even a fresh nerve so she'll be able to feel it," Johnson said on the US Army's website. Burrage, a 21-year-old private, still has to endure two more surgeries, but she's feeling more optimistic about the future than ever in the years since her accident. "It's been a long process for everything, but I'm back," said Burrage.
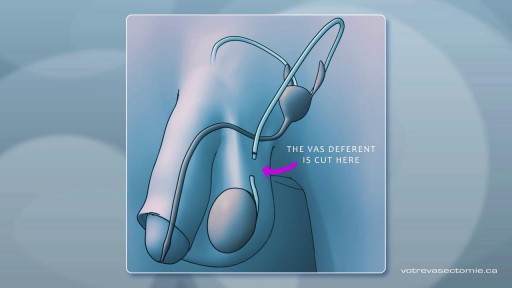
A vasectomy is one of the most effective kinds of birth control out there, and THE most effective method for people with penises and testicles. Vasectomies are almost 100% effective at preventing pregnancy — but not right away. It takes about 3 months for your semen to become sperm-free
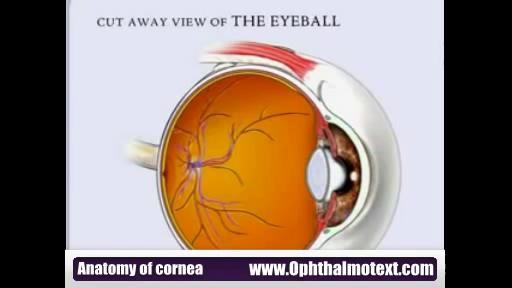
In dark or dim light, the pupil dilates to allow more light into the eye to improve vision. Normal pupil size tends to range between 2.0 and 5.0 millimeters, depending on the lighting. The younger you are, the larger your pupils tend to be.

How to Teach Kids to Safely Lift, Carry and Move Heavy Objects

Curious about physiotherapy or wanting to know how to properly perform an exercise? Check us out on Social Media! Facebook: https://www.facebook.com/striveptandperformance/ Instagram: https://www.instagram.com/striveptandperf/ Twitter: https://twitter.com/StrivePTandPerf Blog: http://www.strivept.ca/blog

Median Sternotomy performed before open heart surgery !

Every day, specialists deliver high-quality care in 68 disciplines in health centres across Canada. Yet many Canadians know very little about what many specialists actually do, and the important role these disciplines play in Canada’s health care system.

What are the classifications of burns? Burns are classified as first-, second-, or third-degree, depending on how deep and severe they penetrate the skin's surface. First-degree (superficial) burns. First-degree burns affect only the epidermis, or outer layer of skin. The burn site is red, painful, dry, and with no blisters. Mild sunburn is an example. Long-term tissue damage is rare and usually consists of an increase or decrease in the skin color. Second-degree (partial thickness) burns. Second-degree burns involve the epidermis and part of the dermis layer of skin. The burn site appears red, blistered, and may be swollen and painful. Third-degree (full thickness) burns. Third-degree burns destroy the epidermis and dermis and may go into the subcutaneous tissue. The burn site may appear white or charred Fourth degree burns. Fourth degree burns also damage the underlying bones, muscles, and tendons. There is no sensation in the area since the nerve endings are destroyed.
The oral contraceptive pill, commonly known as "the pill," is a hormone-based method of preventing pregnancy. It can also help resolve irregular menstruation, painful or heavy periods, endometriosis, acne, and premenstrual syndrome (PMS). Birth control pills work by preventing ovulation. No egg is produced, so there is nothing for the sperm to fertilize. Pregnancy cannot occur. "The pill" is used by nearly 16 percent of women aged 15 to 44 years in the United States, and it has both advantages and disadvantages. People with different risk factors may be advised to use a particular kind of pill. There are different types of contraceptive pills. They all contain synthetic forms of the hormones estrogen, progesterone, or both. Synthetic progesterone is called progestin. Combination pills contain progestin and estrogen. The "mini pill," contains only progestin. Monophasic pills all contain the same balance of hormones. With phasic pills, two or three different types of pill are taken each month, each with a different balance of hormones.
ESCLEROTERAPIA

A walk through of an interactive about male to female sex reassignment surgery.

Treatment consists of diet modifications and laxatives A high-fiber diet can be effective, along with over-the-counter medications, such as stool softeners. In some cases, a medical procedure to remove the hemorrhoid may be needed to provide relief.

very day, specialists deliver high-quality care in 68 disciplines in health centres across Canada. Yet many Canadians know very little about what many specialists actually do, and the important role these disciplines play in Canada’s health care system. This video provides a brief high-level overview of what Internal Medicine Specialists actually do, their training, and their role in Canadian health care.

Tummy tuck surgery, also known as abdominoplasty, removes excess fat and skin and, in most cases, restores weakened or separated muscles creating an abdominal profile that is smoother and firmer. A flat and well-toned abdomen is something many of us strive for through exercise and weight control. Sometimes these methods cannot achieve our goals. Even individuals of otherwise normal body weight and proportion can develop an abdomen that protrudes or is loose and sagging. The most common causes of this include: Aging Heredity Pregnancy Prior surgery Significant fluctuations in weight What tummy tuck surgery can't do A tummy tuck is not a substitute for weight loss or an appropriate exercise program. Although the results of a tummy tuck are technically permanent, the positive outcome can be greatly diminished by significant fluctuations in your weight. For this reason, individuals who are planning substantial weight loss or women who may be considering future pregnancies would be advised to postpone a tummy tuck. A tummy tuck cannot correct stretch marks, although these may be removed or somewhat improved if they are located on the areas of excess skin that will be excised.

A fractured rib is usually a result of a fall or accident. Prolonged coughing and sports with repetitive movement, such as golf, also can cause a rib fracture. Symptoms include pain when taking a deep breath, pressing on the injured area, or bending or twisting the body. In most cases, fractured ribs usually heal on their own in one or two months. Pain relievers can make it easier to breathe deeply.

Manipulation L5/S1 Lumbar Roll and Sacroiliac joint Sidelying

Ectopia cordis is a rare genetic defect. During a baby’s development in utero, their chest wall doesn’t form correctly. It also doesn’t fuse together as it normally would. This prevents the heart from developing where it should, leaving it defenseless and exposed outside of the protection of the chest wall. The defect affects about one in 126,000 births. In partial ectopia cordis, the heart is located outside the chest wall, but just under the skin. The heart can be seen beating through the skin.
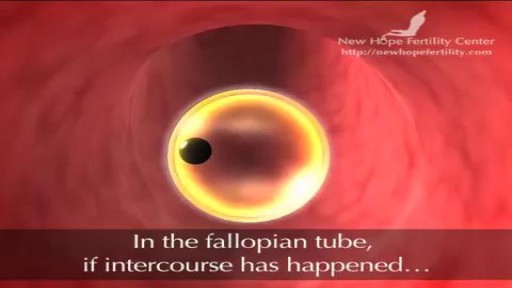
Before ovulation occurs, the average diameter of the dominant follicle is 22 to 24 mm (range 18-36 mm). It is the only marker that can predict ovulation with ease. * In stimulated cycle (hormonal treatment), generally, all or most of the antral follicles grow. The growth rate will be different for each of them.

Bullae resection for right pneumothrax via VATS
