- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
How to Get Rid of Mucus in Lungs
MENTAL STATUS EXAMINATION
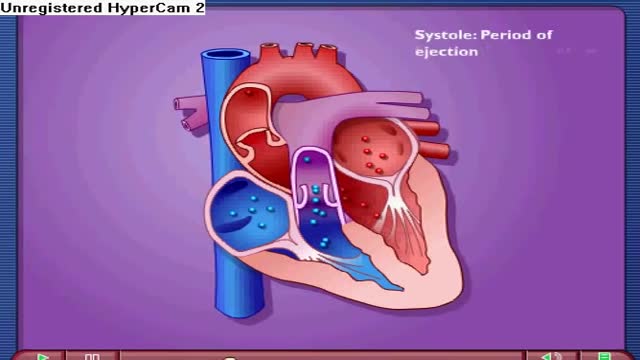
Near the end of diastole, the ventricles nearly fill with blood, and then the atria contract, adding even more volume to the ventricles. The volume of blood in the ventricles at the end of diastole is referred to as the end-diastolic volume. The other phase of the cardiac cycle is called systole.

A colostomy is an operation that creates an opening for the colon, or large intestine, through the abdomen. A colostomy may be temporary or permanent. It is usually done after bowel surgery or injury.
Triglycerides are a type of fat (lipid) found in your blood. When you eat, your body converts any calories it doesn't need to use right away into triglycerides. The triglycerides are stored in your fat cells. Later, hormones release triglycerides for energy between meals. If you regularly eat more calories than you burn, particularly "easy" calories like carbohydrates and fats, you may have high triglycerides (hypertriglyceridemia).
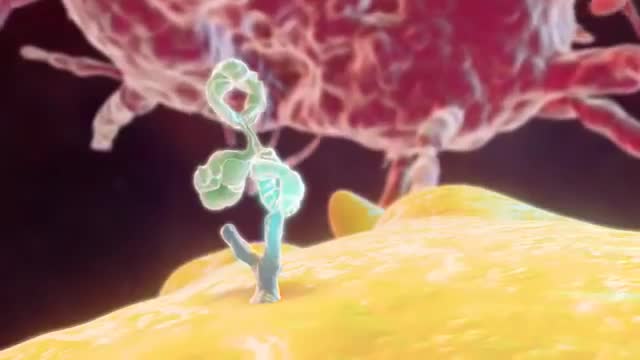
A new report analyzing FDA-approved monoclonal antibodies (mAbs) produced by a select group of leading biotechnology companies shows that clinical development times – specifically the duration of Phase II and Phase III trials – are lengthening, while FDA review times have remained constant. The average time from investigational new drug (IND) filing to market was 6.7 years for 11 mABs approved between 1994 and 2003 but shot up to 8.3 years for 12 mAbs approved between 2004 and March 9, 2011, according to Deloitte Recap LLC’s analysis, Therapeutic Monoclonal Antibodies – Insights, Strategies and Data.

The easy experimental answer to this question is 264 hours (about 11 days). In 1965, Randy Gardner, a 17-year-old high school student, set this apparent world-record for a science fair. Several other normal research subjects have remained awake for eight to 10 days in carefully monitored experiments. None of these individuals experienced serious medical, neurological, physiological or psychiatric problems. On the other hand, all of them showed progressive and significant deficits in concentration, motivation, perception and other higher mental processes as the duration of sleep deprivation increased. Nevertheless, all experimental subjects recovered to relative normality within one or two nights of recovery sleep. Other anecdotal reports describe soldiers staying awake for four days in battle, or unmedicated patients with mania going without sleep for three to four days.

The timing of the nausea or vomiting can indicate the cause. When appearing shortly after a meal, nausea or vomiting may be caused by food poisoning, gastritis (inflammation of the stomach lining), an ulcer, or bulimia. Nausea or vomiting one to eight hours after a meal may also indicate food poisoning.
-Almost all the cases of occupational transmission of HIV have been due to transmission via exposure to blood and certain body fluids. The body fluids wherein standard precautions have been recommended include semen, vaginal secretions, and any other body fluid containing visible blood. Other standard precautions, according to the Center for Disease Control and Prevention (CDC), also apply to cerebrospinal, peritoneal, pleural, pericardia!, synovial fluid, or any other tissue, even though the epidemiologic data regarding the risk of HIV transmission from these fluids is insufficient. Standard precautions do not apply to urine, sweat, tears, sputum, vomitus, and nasal secretions or feces, as long as there is no gross visible blood. The occupational transmission of HIV has never been documented from the above sources.
This is a video on allergic mechanism in our body.this animation video shows how allergens come in contact and how does the body react to such allergens and what is the effect of anti histamine drugs over these allergens.

The Hydatid cyst in the video weighed approximately 300gms and had a diameter of 9 cms .
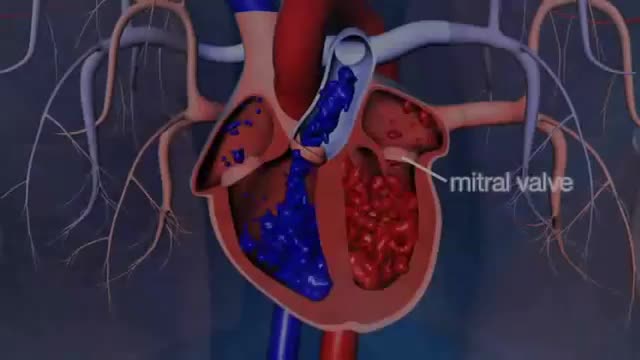
Dr. Glenn Barnhart explains the symptoms of mitral valve regurgitation such as becoming short of breath. There are five structures of the mitral valve: annulus, leaflet tissue, chordae tendineae, papillary muscles, and left ventricle. All of these are taken into consideration when the mitral valve is leaking and not working right. There are four degrees of mitral valve regurgitation: mild, moderate, moderately severe,.
Dr Sergio Canavero, believes he can successfully perform the world's first human head transplant in 2017. Within the medical establishment there is concern and scepticism—but either way the operation is set to be one of the big talking points of the year ahead.
Smallpox disease is a serious, highly contagious, and often life-threatening infection marked by a rash of round pox (blisters) on the face, arms, and legs. It is caused by the Variola virus. The last case of smallpox in the United States was in 1949.

Markle Test (heel jar test) for Peritonitis
Super Obese individuals (people with a Body Mass Index over 45) have an increased risk during any surgery. And the longer the time under anesthesia, the greater the risk. Gastric bypass surgery can last over 2 hours. Duodenal switch surgery often takes over 4 hours. That’s a long time to be under anesthesia.

Aim: To detail two different clinical protocols and case studies using mini-implant anchorage developed to respond to certain clinical conditions. Methods: Two clinical protocols are described to upright mesially tilted mandibular molars. In the first protocol, a single mini-implant is inserted distally to the molar to be uprighted, and an elastic traction chain is applied to the tooth. In the second clinical approach, two mini-implants are inserted mesially. A screw-suspended TMA sectional archwire is applied (Derton-Perini technique). Two cases, descriptive of the two different treatment protocols, are described. In the first case, the mandibular right second premolar was missing and the adjacent first molar needed to be uprighted. A single screw was inserted distally to the first molar, and an elastic chain was applied. In the second case, the mandibular left second molar was missing and the third molar needed to be uprighted. Two mini-implants were inserted mesially and a fully screw-supported sectional archwire was used to upright and bodily mesialize the third molar. Results: Both uprighting approaches uprighted the molar axis without loss of anchorage. Conclusion: The two approaches to mandibular molar uprighting, developed as rational responses to different clinical cases, were both found to be effective. Research paper: Mandibular molar uprighting using mini-implants: Different approaches for different clinical cases-Two case reports.. Available from: https://www.researchgate.net/publication/224920305_Mandibular_molar_uprighting_using_mini-implants_Different_approaches_for_different_clinical_cases-Two_case_reports [accessed

This device can detect several diseases from a single drop of blood.
Pernicious anemia Email this page to a friend Print Facebook Twitter Google+ Anemia is a condition in which the body does not have enough healthy red blood cells. Red blood cells provide oxygen to body tissues. There are many types of anemia. Pernicious anemia is a decrease in red blood cells that occurs when the intestines cannot properly absorb vitamin B12.
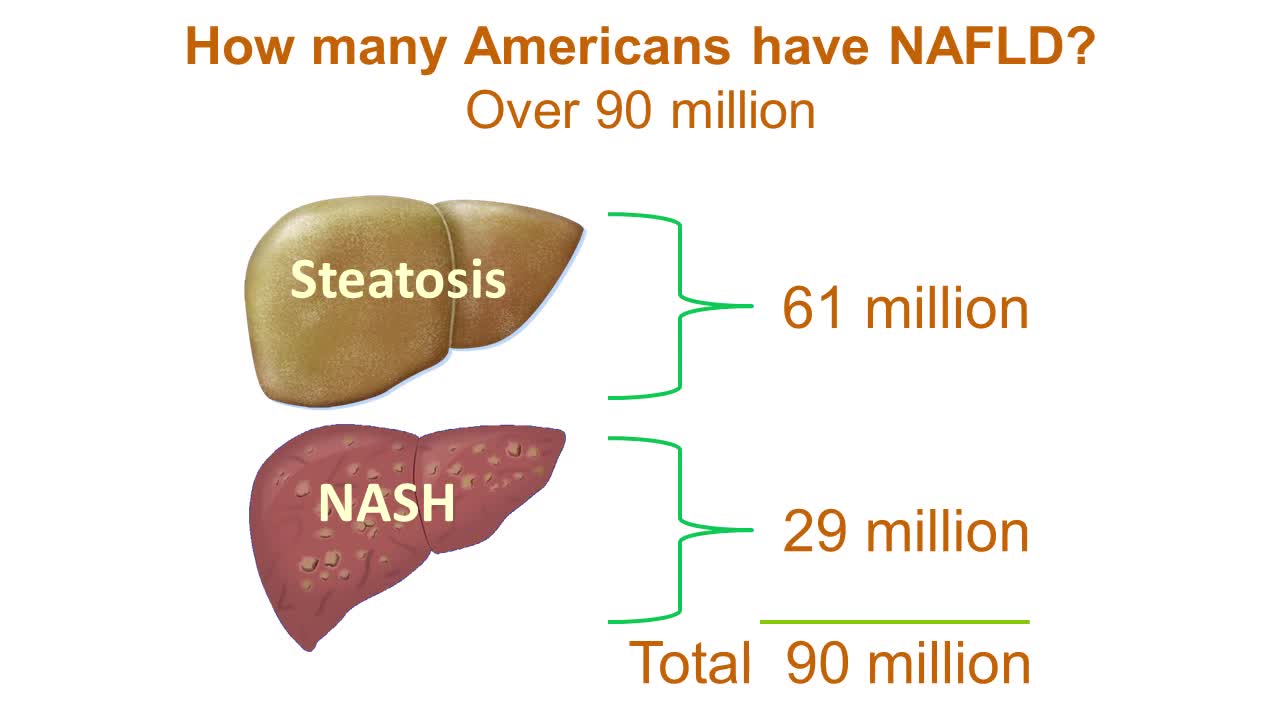
Nonalcoholic fatty liver disease is an umbrella term for a range of liver conditions affecting people who drink little to no alcohol. As the name implies, the main characteristic of nonalcoholic fatty liver disease is too much fat stored in liver cells. Nonalcoholic steatohepatitis, a potentially serious form of the disease, is marked by liver inflammation, which may progress to scarring and irreversible damage. This damage is similar to the damage caused by heavy alcohol use. At its most severe, nonalcoholic steatohepatitis can progress to cirrhosis and liver failure Nonalcoholic fatty liver disease is increasingly common around the world, especially in Western nations. In the United States, it is the most common form of chronic liver disease, affecting an estimated 80 to 100 million people. Nonalcoholic fatty liver disease occurs in every age group but especially in people in their 40s and 50s who are at high risk of heart disease because of such risk factors as obesity and type 2 diabetes. The condition is also closely linked to metabolic syndrome, which is a cluster of abnormalities including increased abdominal fat, poor ability to use the hormone insulin, high blood pressure and high blood levels of triglycerides, a type of fat. Nonalcoholic fatty liver disease care at Mayo Clinic Request an Appointment at Mayo Clinic Symptoms & causes Aug. 23, 2016 Print Share on: Facebook Twitter References Related Magnetic resonance elastography Nonalcoholic fatty liver disease Overview Symptoms & causes Diagnosis & treatment Diagnosis Treatment Departments & specialties Expertise & rankings Locations, travel & lodging Clinical trials Research Costs & insurance Preparing for your appointment Self-management More about In-Depth Multimedia Resources News from Mayo Clinic Advertisement
