- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
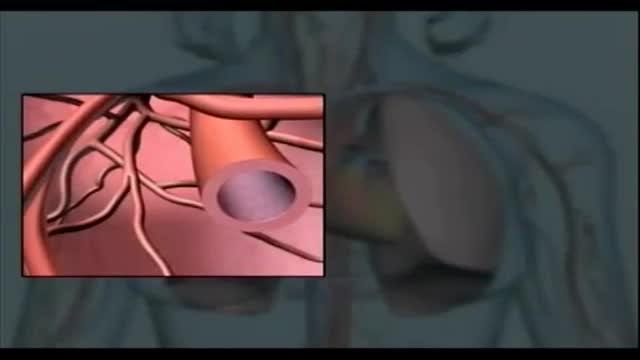
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Your body's immune system protects you from disease and infection. But if you have an autoimmune disease, your immune system attacks healthy cells in your body by mistake. Autoimmune diseases can affect many parts of the body. No one is sure what causes autoimmune diseases. They do tend to run in families. Women - particularly African-American, Hispanic-American, and Native-American women - have a higher risk for some autoimmune diseases. There are more than 80 types of autoimmune diseases, and some have similar symptoms. This makes it hard for your health care provider to know if you really have one of these diseases, and if so, which one. Getting a diagnosis can be frustrating and stressful. Often, the first symptoms are fatigue, muscle aches and a low fever. The classic sign of an autoimmune disease is inflammation, which can cause redness, heat, pain and swelling. The diseases may also have flare-ups, when they get worse, and remissions, when symptoms get better or disappear. Treatment depends on the disease, but in most cases one important goal is to reduce inflammation. Sometimes doctors prescribe corticosteroids or other drugs that reduce your immune response.

► Sign up here and try our FREE content: http://lectur.io/freecontentyt
► If you’re an medical educator or faculty member, visit: http://lectur.io/medytb2u
This video “Epithelium” is part of the Lecturio course “Histology” ► WATCH the complete course on http://lectur.io/epithelium
► LEARN ABOUT:
- Introduction: Epithelial Tissue
- Summary of structure and function
- Epithelium
- Three characteristics of any Epithelium
- Epithelium: Classification
- Epithelium: Epithelial Cells Exhibit Polarity
- Epithelium: How Are Epithelial Cells Joined Together?
- Epithelium: Surfaces of Epithelial Cells
- Epithelium: Basement Membrane
► THE PROF: Your lecturer is Professor Geoff Meyer. He is currently teaching at the School of Anatomy, Physiology and Human Biology at the University of Western Australia (UWA). As a leading anatomy and histology expert he is also coordinating the Federative International Program for Anatomical Terminologies (FIPAT) of the International Federation of Associations of Anatomists (IFAA). Besides medical research on the ovarian function, steroidogenesis, corpus luteum, angiogenesis, and microcirculation, Geoff Meyer’s research activities also focus on developing innovative, computer-aided learning and teaching tools. For his inventiveness, Geoff Meyer has received a number of awards, including the Australian University Teaching Award.
► LECTURIO is your single-point resource for medical school:
Study for your classes, USMLE Step 1, USMLE Step 2, MCAT or MBBS with video lectures by world-class professors, recall & USMLE-style questions and textbook articles. Create your free account now: http://lectur.io/epithelium
► INSTALL our free Lecturio app
iTunes Store: https://app.adjust.com/z21zrf
Play Store: https://app.adjust.com/b01fak
► READ TEXTBOOK ARTICLES related to this video:
Epithelium — Functions and Types of Epithelial Tissue
http://lectur.io/epitheliumarticle
► SUBSCRIBE to our YouTube channel: http://lectur.io/subscribe
► WATCH MORE ON YOUTUBE: http://lectur.io/playlists
► LET’S CONNECT:
• Facebook: https://www.facebook.com/lectu....rio.medical.educatio
• Instagram: https://www.instagram.com/lecturio_medical_videos
• Pinterest: https://www.pinterest.de/lecturiomedical
• LinkedIn: https://www.linkedin.com/company/lecturio-medical/
Anaphylaxis is a severe, potentially life-threatening allergic reaction. It can occur within seconds or minutes of exposure to something you're allergic to, such as a peanut or the venom from a bee sting. The flood of chemicals released by your immune system during anaphylaxis can cause you to go into shock; your blood pressure drops suddenly and your airways narrow, blocking normal breathing. Signs and symptoms of anaphylaxis include a rapid, weak pulse, a skin rash, and nausea and vomiting. Common triggers of anaphylaxis include certain foods, some medications, insect venom and latex. Anaphylaxis requires an immediate trip to the emergency department and an injection of epinephrine. If anaphylaxis isn't treated right away, it can lead to unconsciousness or even death.

Endometrial cancer is a type of cancer that begins in the uterus. The uterus is the hollow, pear-shaped pelvic organ in women where fetal development occurs. Endometrial cancer begins in the layer of cells that form the lining (endometrium) of the uterus. Endometrial cancer is sometimes called uterine cancer. Other types of cancer can form in the uterus, including uterine sarcoma, but they are much less common than endometrial cancer. Endometrial cancer is often detected at an early stage because it frequently produces abnormal vaginal bleeding, which prompts women to see their doctors. If endometrial cancer is discovered early, removing the uterus surgically often cures endometrial cancer.

INVIVO

If they are damaged, waste and fluids build up in your blood instead of leaving your body. Kidney damage from diabetes is called diabetic nephropathy. It begins long before you have symptoms. An early sign of it is small amounts of protein in your urine.

Technically, there's no formal definition for a "Code", but doctors often use the term as slang for a cardiopulmonary arrest happening to a patient in a hospital or clinic, requiring a team of providers (sometimes called a "code team") to rush to the specific location and begin immediate resuscitative efforts.
Breast lump removal is surgery to remove a lump that may be breast cancer. Tissue around the lump is also removed. This surgery is called a lumpectomy. When a noncancerous tumor such as a fibroadenoma of the breast is removed, it is often called an excisional breast biopsy, instead of a lumpectomy

Neonatal resuscitation skills are essential for all health care providers who are involved in the delivery of newborns. The transition from fetus to newborn requires intervention by a skilled individual or team in approximately 10% of all deliveries. This figure is concerning because 81% of all babies in the United States are born in nonteaching, nonaffiliated level I or II hospitals. In such hospitals, the volume of delivery service may not be perceived as sufficient economic justification for the continuous in-hospital presence of personnel with high-risk delivery room experience, as recommended by the American Academy of Pediatrics (AAP) and the American College of Obstetricians and Gynecologists (ACOG). [1] Perinatal asphyxia and extreme prematurity are the 2 complications of pregnancy that most frequently necessitate complex resuscitation by skilled personnel. However, only 60% of asphyxiated newborns can be predicted ante partum. The remaining newborns are not identified until the time of birth. Additionally, approximately 80% of low-birth-weight infants require resuscitation and stabilization at delivery. Nearly one half of newborn deaths (many of which involve extremely premature infants) occur during the first 24 hours after birth. Many of these early deaths also have a component of asphyxia or respiratory depression as an etiology. For the surviving infants, effective management of asphyxia in the first few minutes of life may influence long-term outcome. Even though prenatal care can identify many potential fetal difficulties ante partum, allowing maternal transfer to the referral center for care, many women who experience preterm labor are not identified prospectively and therefore are not appropriately transferred to a tertiary perinatal center. Consequently, many deliveries of extremely premature infants occur in smaller hospitals. For this reason, all personnel involved in delivery room care of the newborn should be trained adequately in all aspects of neonatal resuscitation. Additionally, equipment that is appropriately sized to resuscitate infants of all gestational ages should be available in all delivering institutions, even if the institution does not care for preterm or intensive care infants. Along with the necessary skills, the practitioner should approach any resuscitation with a good comprehension of transitional physiology and adaptation, as well as an understanding of the infant's response to resuscitation. Resuscitation involves much more than possessing an ordered list of technical skills and having a resuscitation team; it requires excellent assessment skills and a grounded understanding of physiology.

In these times when there are uncountable online pharmacies being recognized, mynetpharma.com stands out as one of the best.The drug catalogue of this web pharmacy has medicines to treat a range of health issues ranging from medicines to treat obesity, alopecia, allergy, bacterial infections, pain etc. Mynetpharma(http://www.mynetpharma.com) provide a range of top quality medicines to their customers who are based in different parts of the world to help them overcome their health problems.

Celebrity hair stylist Michael DeMarse of Houston, TX shares his experience with us. Michael has been a loyal patient of Dr. Jue for a long time! Call us for a free consultation at (281) 277-9200 or visit https://www.sugarlanddentalspa.com/
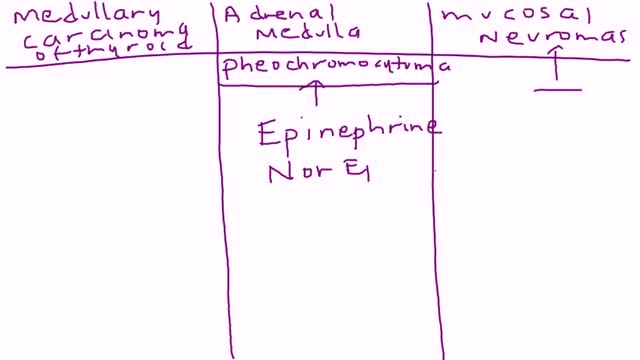
Multiple endocrine neoplasia type 2 (MEN2) is a hereditary condition associated with three primary types of tumors: medullary thyroid cancer, parathyroid tumors, and pheochromocytoma. MEN2 is classified into three subtypes based on clinical features. MEN2A, which affects 60% to 90% of MEN2 families Medullary thyroid cancer: 98% to 100% with MEN2A are affected Pheochromocytoma, a typically benign (noncancerous) tumor of the adrenal glands: 50% with MEN2A affected Parathyroid adenoma (benign tumor) or hyperplasia, meaning increased size, of the parathyroid gland: 5% to 10% with MEN2A affected MEN2B, which affects 5% of MEN2 families Medullary thyroid cancer: 98% to 100% with MEN2B affected Pheochromocytoma: 50% with MEN2B affected Mucosal neuromas, which is a benign tumor of nerve tissue on the tongue, lips and throughout the gastrointestinal tract: 95% to 98% affected Digestive problems caused by disordered nerves in the gastrointestinal tract: 75% to 90% affected Muscle, joint, and spinal problems: 95% affected Typical facial features, including swollen lips and thick eyelids: 75% to 90% affected Familial medullary thyroid cancer (FMTC), which affects 5% to 35% of MEN2 families Medullary thyroid carcinoma only Sources: Gagel RF, Marx SJ. “Multiple endocrine neoplasia.” Williams Textbook of Endocrinology, Chapter 40, 11th ed., Philadelphia, 2008, and Eng C, Clayton D, et al. Grubbs EG, Gagel RF. My, How Things Have Changed in Multiple Endocrine Neoplasia Type 2A! J Clin Endocrinol Metab 100(7):2532-5, 7/2015. PMID: 26151398. What causes MEN2? MEN2 is a genetic condition. This means that the cancer risk and other features of MEN2 can be passed from generation to generation in a family. The gene associated with MEN2 is called RET. A mutation (alteration) in the RET gene gives a person an increased risk of developing medullary thyroid cancer and other tumors associated with MEN2.
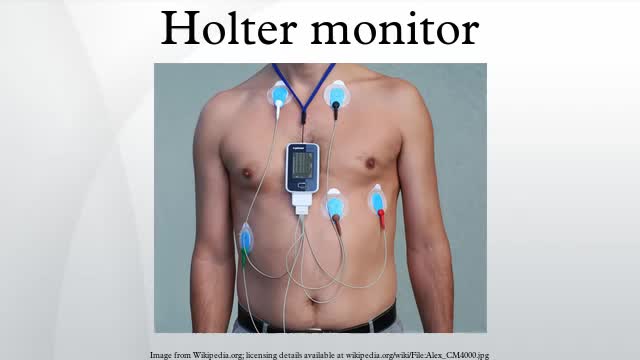
Holter monitoring, electrocardiogram or echocardiogram are only recommended if a cardiac cause (e.g., arrhythmias, possible cardiac syncope, myocardial ischemia) is suspected.
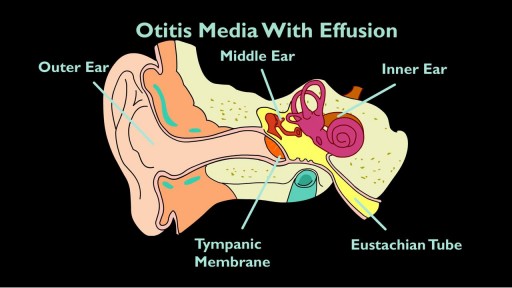
The eustachian tube drains fluid from your ears to the back of your throat. If it clogs, otitis media with effusion (OME) can occur. If you have OME, the middle part of your ear fills with fluid, which can increase the risk of ear infection. OME is very common. According to the Agency of Healthcare Research and Quality, about 90 percent of children will have OME at least once by the age of 10.

Arthrocentesis involves both the puncture of a joint and the aspiration of its synovial fluid. It is typically used to make an accurate diagnosis of a painful, warm, swollen joint. Removal of excess fluid can be therapeutic. Analysis of the removed fluid helps to decipher its etiology. [1]
Most of the time, you won't know the exact day you got pregnant. Your doctor will count the start of your pregnancy from the first day of your last menstrual period. That's about 2 weeks ahead of when conception happens.

The journey of egg and sperm. There are a lot of casualties (deaths) among the sperm as they swim toward the egg. First, many get lost in the maze of a woman's uterus where they also have to contend with acidic vaginal secretions.

Temporary Anchorage Device (TAD) - Orthodontic Device, very impressive
Endotracheal intubation is a medical procedure in which a tube is placed into the windpipe (trachea) through the mouth or nose. In most emergency situations it is placed through the mouth. Whether you are awake (conscious) or not awake (unconscious), you will be given medicine to make it easier to insert the tube. After endotracheal intubation, you will likely be placed on a breathing machine. If you are awake after the procedure, your health care provider may give you medicine to reduce your anxiety or discomfort.
