- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Aim: To detail two different clinical protocols and case studies using mini-implant anchorage developed to respond to certain clinical conditions. Methods: Two clinical protocols are described to upright mesially tilted mandibular molars. In the first protocol, a single mini-implant is inserted distally to the molar to be uprighted, and an elastic traction chain is applied to the tooth. In the second clinical approach, two mini-implants are inserted mesially. A screw-suspended TMA sectional archwire is applied (Derton-Perini technique). Two cases, descriptive of the two different treatment protocols, are described. In the first case, the mandibular right second premolar was missing and the adjacent first molar needed to be uprighted. A single screw was inserted distally to the first molar, and an elastic chain was applied. In the second case, the mandibular left second molar was missing and the third molar needed to be uprighted. Two mini-implants were inserted mesially and a fully screw-supported sectional archwire was used to upright and bodily mesialize the third molar. Results: Both uprighting approaches uprighted the molar axis without loss of anchorage. Conclusion: The two approaches to mandibular molar uprighting, developed as rational responses to different clinical cases, were both found to be effective. Research paper: Mandibular molar uprighting using mini-implants: Different approaches for different clinical cases-Two case reports.. Available from: https://www.researchgate.net/publication/224920305_Mandibular_molar_uprighting_using_mini-implants_Different_approaches_for_different_clinical_cases-Two_case_reports [accessed

This device can detect several diseases from a single drop of blood.
Pernicious anemia Email this page to a friend Print Facebook Twitter Google+ Anemia is a condition in which the body does not have enough healthy red blood cells. Red blood cells provide oxygen to body tissues. There are many types of anemia. Pernicious anemia is a decrease in red blood cells that occurs when the intestines cannot properly absorb vitamin B12.
This video describe the clinical managment of a patient with hyperprolactinemia, including the approach to diagnosis, important endocrine testing, and management options.
A heart attack is a frightening experience. If you have had a heart attack, or are close with someone who has, you are not alone: tens of thousands of Americans survive. As you work toward recovery, please use the following questions and answers to better understand what has happened to you and how you can help your heart heal so you can live a healthier, longer life.
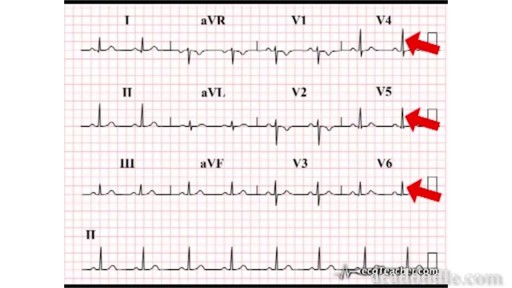
Learn the basics of ECG (EKG) in one minute
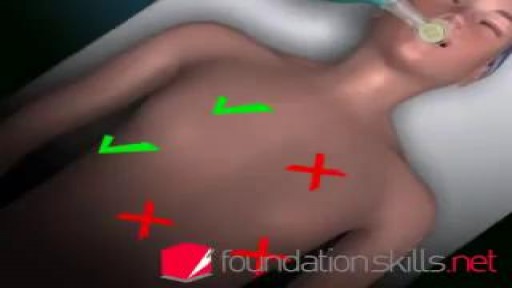
Endotracheal intubation is a medical procedure in which a tube is placed into the windpipe (trachea) through the mouth or nose. In most emergency situations it is placed through the mouth. Whether you are awake (conscious) or not awake (unconscious), you will be given medicine to make it easier to insert the tube. After endotracheal intubation, you will likely be placed on a breathing machine. If you are awake after the procedure, your health care provider may give you medicine to reduce your anxiety or discomfort.

Occlusal Stamp Technique.Make Occlusal Anatomy Easily

3D printing a titanium vertebrae
A reconstructive transplant, also called a composite tissue transplant or composite tissue allograft, is an operation that involves transplantation of bone, tissue, muscle and blood vessels. A reconstructive hand transplant is an operation tailored to each patient’s individual needs, type of injury and anatomy. This transplants an upper extremity, usually at the level of the forearm and wrist, but sometimes above the elbow, to help restore function after the loss of a hand or arm.

Carpal tunnel release is a surgery used to treat and potentially heal the painful condition known as carpal tunnel syndrome. Doctors used to think that carpal tunnel syndrome was caused by an overuse injury or a repetitive motion performed by the wrist or hand, often at work. They now know that it’s most likely a congenital predisposition (something that runs in families) – some people simply have smaller carpal tunnels than others. Carpal tunnel syndrome can also be caused by injury, such as a sprain or fracture, or repetitive use of a vibrating tool. It's also been linked to pregnancy, diabetes, thyroid disease, and rheumatoid arthritis.
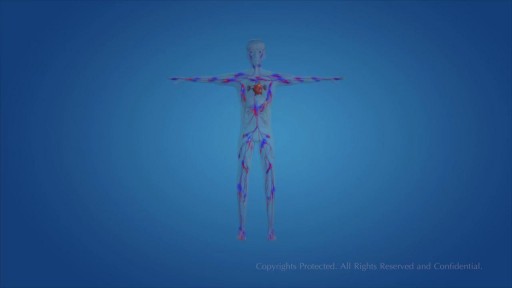
Human Circulatory System and heart video
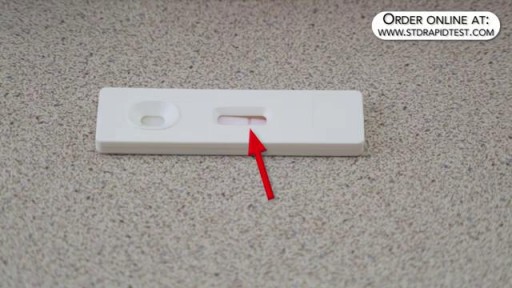
How to use a Gonorrhea rapid test kit for self-diagnosis of Gonorrhea (swab test). Convenient, Easy to Use, and over 99% Accurate. Certified GMP and ISO13485. Test yourself at home with Complete Privacy. Buy online today at: http://www.stdrapidtest.com
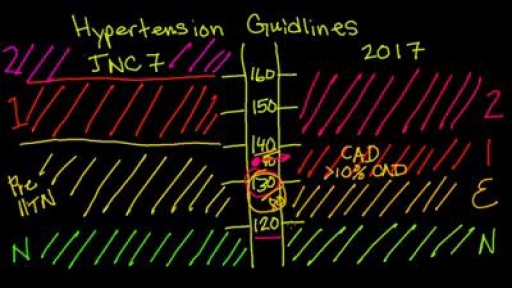
New 2017 Hypertension guidelines

Watch that video to know How to Shape Your Saggy Breasts Naturally
What Is Phonemic Awareness, Reading Program For Kids, Phonics For Children, Teach Your Baby To Read---- http://children-learning-reading.good-info.co----- What is Phonemic Awareness, Phonemic Awareness is defined as the ability to identify, hear, and work with the smallest units of sound known as phonemes. It is NOT the same as phonological awareness, instead, it is a sub-category of phonological awareness. For example, phonemic awareness is narrow, and deals only with phonemes and manipulating the individual sounds of words - such as /c/, /a/, and /t/ are the individual sounds that make up to form the word "cat". Phonological awareness on the other hand, includes the phonemic awareness ability, and it also includes the ability to hear, identify, and manipulate larger units of sound such as rimes and onsets. Phonemic awareness can be taught very early on, and will play a critical role in helping children learn to read and spell. While it's not set in stone on when a child can learn to read, however, I do believe that a child that can speak is a child that can learn to read. Children as young as two years old can learn to read by developing phonemic awareness, and they can learn to read fluently. Please see a video of a 2 year old (2yr11months) reading below. Below are several of the most common phonemic awareness skills that are often practiced with students and young children: Phonemic identity - being able to recognize common sounds in different words such as /p/ is the common sound for "pat", "pick", and "play". Phonemic isolation - being able to recognize the individual sounds of words such as /c/ is the beginning sound of "cat" and /t/ is the ending sound of "cat". Phoneme substitution - being able to change one word to another by substituting one phoneme. For example changing the /t/ in "cat" to /p/ now makes "cap". Word Segmenting - the parent says the word "lap", and the child says the individual sounds: /l/, /a/, and /p/. Oral blending - the parent says the individual sounds such as /r/, /e/, and /d/, and the child forms the word from the sounds to say "red". Studies have found that phonemic awareness is the best predictor of reading success in young children. Research has also found that children with a high level of phonemic awareness progress with high reading and spelling achievements; however, some children with low phonemic awareness experience difficulties in learning to read and spell. Therefore, it is important for parents to help their young children develop good phonemic awareness. Being able to oral blend and segment words helps children to read and spell. According to the National Reading Panel, oral blending helps children develop reading skills where printed letters are turned into sounds which combine to form words. Additionally, word segmenting helps children breakdown words into their individual sounds (phonemes), and helps children learn to spell unfamiliar words. As a young child begins to develop and master phonemic awareness skills, they will discover an entirely new world in print and reading. You will open up their world to a whole new dimension of fun and silliness. They will be able to read books that they enjoy, develop a better understanding of the world around them through printed materials, and have a whole lot of fun by making up new nonsense words through phonemic substitutions. For example, we taught our daughter to read at a young age - when she was a little over 2 and a half years old. Before she turned three, she would run around the house saying all types of silly words using phonemic substitution. One of her favorite was substituting the letter sound /d/ in "daddy" with the letter sound /n/. So, she would run around me in circles and repeatedly say "nanny, nanny, come do this" or "nanny, nanny, come play with me" etc... Of course, she only did this when she wanted to be silly and to make me laugh, at other times, she would of course properly refer to me as "daddy", and not "nanny". She is well aware of the differences between these words and is fully capable of using phonemic substitution to change any of the letters in the words to make other words. Give your child a head start, and.. pave the way for a bright, successful future..Click here to learn how to easily and quickly teach your child to read. http://children-learning-reading.good-info.co

Watch that Above Knee Leg Amputation Medical Surgery

Hip replacement is a surgical procedure in which the hip joint is replaced by a prosthetic implant, that is, a hip prosthesis. Hip replacement surgery can be performed as a total replacement or a hemi replacement

Surgery is performed by Kami Parsa M.D. The patient is a 55 year old with a history of previous upper eyelid blepharoplasty with excessive skin removed from both upper eyelids which resulted in bilateral lagophthalmos. Patient could not close her eyes and had problems with severe dry eyes.

Many people have baggy and puffy lower eyelids. Lower Eyelid Surgery (Blepharoplasty) is the removal of excess fat and tightening of the skin, which can drastically minimize the appearance of baggy and puffy lower eyelids that makes everyone look tired and worn down. This procedure is just as popular with men as with women. A sense of well-being and alertness is the reason why most people elect to have this procedure. Lower lids surgery is a procedure that the best results are achieved when performed earlier than later. Dr. Lee has performed this surgery on patients who are 18 yrs old to 82 yrs old- all very happy with their results. The cause of baggy and puffy lower eyelid is due to a combination of herniating fat, excessive skin, and edema (water retention).
