- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Davinci Robotic Prostatectomy Animation
French Insuficiencia cardiaca

http://www.landging.com/respiratory-circulatory-system-animation.html
Human body circulatory system and respiratory system, 3D MOA (Mechanism of Action) animation, designed for Beijing Natural History Museum.

A new approach to health care working with patients and doctors to streamline the process and makes it easier and more efficient to get health care they need.

http://vaincre-le-diabete.plus101.com
---Traitement Diabete 2. Vous Eliminerez Le Diabète D'Une Fois Pour Toutes!
Laissez de côté les préoccupations des risques de votre maladie.
Ne souffrez plus de votre poids et la privation des aliments préférés.
Ne dépensez plus des milliers d'euros en médicaments qui combattent la maladie de l'extérieur.
Ne vivez plus une vie de restrictions.
Ne souffrez plus!!!
Oubliez de changer constamment de médicaments prescrits, de mesurer le niveau de glucose et de vous injecter l'insuline.
Traitement Diabete 2
http://youtu.be/SvsCAZuKGBo
traitement contre le diabete de type 2,
traitement de diabete type 2,
traitement de diabète de type 2,
traitement diabete type 1,
traitement diabète de type 2,
traitement diabète type 2,
traitement du diabete type 2 par les plantes,
traitement du diabète de type 2,
traitement du diabète par les plantes,
traitement du diabète type 2,
traitement naturel diabete,
traitement pour diabete,
traitement pour le diabète de type 2,
traitements diabète
Hipertension Arterial Pdf, Hipertension Esencial, Hipertension Pulmonar Tratamiento
http://bajar-presion-arterial.good-info.co
Lo Que Todos Necesitan Saber Sobre La Presión Arterial Alta
Si le han dicho que tiene presión arterial alta, usted puede decir, "Pero me siento muy bien!" Esto se debe a que la hipertensión o la presión arterial alta no tiene síntomas visibles. Es por eso que se la describe a menudo como el "asesino silencioso". No hay achaques o limitaciones físicas sólo porque tiene la presión arterial alta. Entonces, por qué siquiera preocuparse?
La hipertensión afecta a uno de cada tres adultos estadounidenses, y muchas de estas personas ni siquiera saben que la tienen. Además, aquellos con presión arterial alta tienen también un mayor riesgo de tener el colesterol alto.
Haga clic en el enlace de abajo para comprobar que funciona
http://bajar-presion-arterial.good-info.co
Suscríbete a nuestro canal
http://bajar-presion-arterial.blogspot.com/
https://www.youtube.com/watch?v=wQU4dgC1FM8
Hipertension Arterial Pdf, Hipertension Esencial, Hipertension Pulmonar Tratamiento,
hipertension renal,
hipertension en embarazo,
hipertension alimentacion,
hipertension arterial diagnostico,
hipertension arterial sistolica,
hipertension remedios naturales,
hipertension pulmonar leve,
hipertension arterial prevencion,
embarazo e hipertension,
diagnostico de hipertension,
sintomas de tension arterial alta,
remedios caseros hipertension

How smoking is causing a hazy filter over your life. Kick cigarettes to the curb for good.

Your kids are going to love brushing! Follow these tips and find out how brushing your teeth can be fun and effective for the whole family.
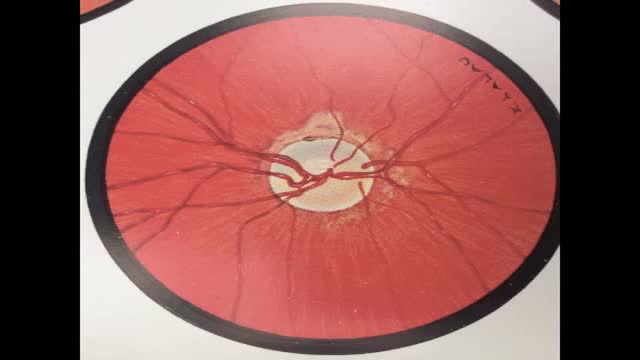
Recent studies show that administration of PEA in glaucoma patients has a double effect, decrease the IOP and neuroprotection. The IOP is the major risk factor in glaucoma, constricts blood vessels and reduces the delivery of oxygen and nutrients to the retina and optic nerve (ON), causing a process of ischemia and cell death (apoptosis).
New research points out palmitoylethanolamide has a dual action in glaucoma:
1. It reduces high eye pressure by promoting fluid flow out of the eye, and
2. PEA protects nerve cells and retina cells via its neuroprotective and reparative properties.
In the Youtube the essence of the natural treatment of glaucoma with palmitoylethanolamide has been summarized. Daily dose: 2-3 times 400 mg palmitoylethanolamide.
Literature on this topic on http://palmitoylethanolamide4pain.com/2015/02/20/youtube-on-palmitoylethanolamide-as-a-natural-treatment-for-glaucoma/

An aortic dissection is a serious condition in which the inner layer of the aorta, the large blood vessel branching off the heart, tears. Blood surges through the tear, causing the inner and middle layers of the aorta to separate (dissect). If the blood-filled channel ruptures through the outside aortic wall, aortic dissection is often fatal. Aortic dissection is relatively uncommon. The condition most frequently occurs in men in their 60s and 70s. Symptoms of aortic dissection may mimic those of other diseases, often leading to delays in diagnosis. However, when an aortic dissection is detected early and treated promptly, the chance of survival greatly improves.

Interstitial cystitis is a clinical syndrome characterized by daytime and nighttime urinary frequency, urgency, and pelvic pain of unknown etiology. Interstitial cystitis has no clear etiology or pathophysiology, and diagnostic criteria for the syndrome remain undefined. Despite considerable research, universally effective treatments do not exist; therapy usually consists of various supportive, behavioral, and pharmacologic measures. Surgical intervention is rarely indicated. The International Continence Society has coined the term painful bladder syndrome (suprapubic pain with bladder filling associated with increased daytime and nighttime frequency, in the absence of proven urinary infection or other obvious pathology) and reserves the diagnosis of interstitial cystitis for patients with characteristic cystoscopic and histologic features of the condition.[1] An international consensus panel was able to generally agree on the following definition of interstitial cystitis/bladder pain syndrome (IC/BPS): unpleasant sensation (pain, pressure, discomfort) perceived to be related to the urinary bladder and associated with lower urinary tract symptoms of more than 6 weeks duration, in the absence of infection or other identifiable causes. American Urological Association (AUA) guidelines published in 2011 and amended in 2014 use an evidence-based approach to provide a clinical framework for the diagnosis and management of this condition.[2, 3, 4] In 1887, Skene initially described a condition characterized by inflammation that destroyed the urinary bladder "mucous membrane partly or wholly and extended to the muscular parietes." Guy Hunner popularized the disease with the description of characteristic bladder wall ulcers in association with a symptom complex of chronic bladder inflammation.[5] The first comprehensive epidemiologic description of interstitial cystitis is credited to Hand, who in 1949 described the widespread, small, submucosal bladder hemorrhages and the significant variation in bladder capacity characteristic of the condition. Despite years of intensive research, there are no specific clinical or urinary markers currently clinically available; no absolutely specific radiographic, laboratory, or serologic findings; and no biopsy patterns that are pathognomonic for interstitial cystitis. Some research suggests that the following may all play a role in the disease pathophysiology: (1) pelvic floor dyfunction, (2) dysregulated immune or inflammatory signals, (3) neural hypersensitivity, and (4) disruption of the proteoglycan/glycosaminoglycan (GAG) layer.[6] Interstitial cystitis, howerver, remains a diagnosis of exclusion (see Presentation, DDx, and Workup.) Intensive study has been done to attempt to identify biomarkers for IC/BPS. Some interesting studies have shown that bladder nitric oxide is an accurate marker for Hunner lesions, but these are not present in all patients, and the test requires specific equipment, which has limited widespread clinical use.[7] Differences in levels of cytokines and chemokines, specifically CXCL-10, have shown some ability to differentiate patients with and without Hunner lesions.[8] Other studies of ulcerative IC/BPS have shown that numerous other cytokines and chemokines are up-regulated as well, heralding a possible urinary test to identify patients.[9] An additional substance shown to be up-regulated in IC/BPS patients is antiproliferative factor (APF). This small 8–amino-acid peptide has been associated with suppression of cell growth, increases in transcellular permeability, and lowering of levels of proteins that form intercellular junctional complexes. It is synthesized and secreted from bladder epithelial cells from patients with IC/BPS and may play a key role in pathophysiology.[10] In vitro studies have shown that removal of APF from cell culture media restored cell proliferation and membrane integrity.[11] Studies have also suggested APF in the therapeutic effect of hydrodistension in patients with IC/BPS, although further confirmatory studies are necessary.[12] The most important element in treating patients with interstitial cystitis is education and emotional support. Periodic exacerbations are managed as they occur because no long-term therapy has been shown to prevent or delay recurrent episodes. Therefore, the purpose of treatment is to palliate and alleviate symptoms. Because no discrete pathognomonic pathologic criteria exist for assessing and monitoring disease severity, indications and goals for treatment are based on the degree of patient symptoms. Assessing patient response to treatment is also complicated because of the subjective nature of symptoms; the waxing and waning nature of symptoms without treatment; and the lack of objective serologic, physical, or histopathologic findings. Conservative measures and oral or intravesical treatments are considered first-line treatment. (See Treatment.)
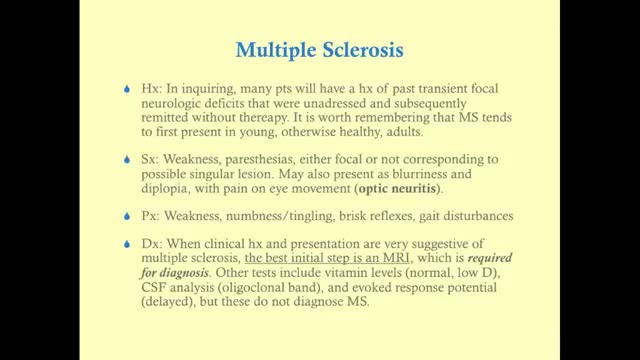
Multiple sclerosis (MS) affects the brain and spinal cord. Early MS symptoms include weakness, tingling, numbness, and blurred vision. Other signs are muscle stiffness, thinking problems, and urinary problems. Treatment can relieve MS symptoms and delay disease progression.

Nipple Sensation After Breast Augmentation
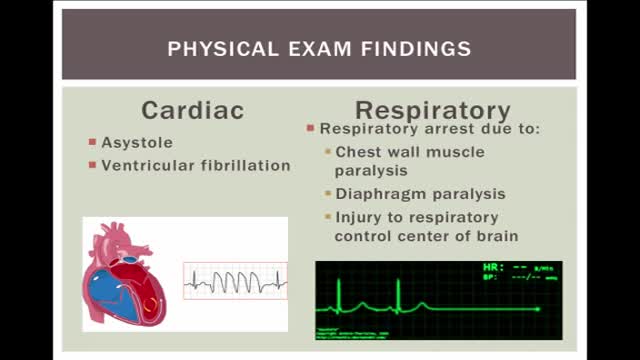
Electrical injuries can present with a variety of problems, including cardiac or respiratory arrest, coma, blunt trauma, and severe burns of several types. It is important to establish the type of exposure (high or low voltage), duration of contact, and concurrent trauma. Low-voltage AC injury without loss of consciousness and/or arrest These injuries are exposures of less than 1000V and usually occur in the home or office setting. Typically, children with electrical injuries present after biting or chewing on an electrical cord and suffer oral burns. Adults working on home appliances or electrical circuits can also experience these electrical injuries. Low-voltage AC may result in significant injury if there is prolonged, tetanic muscle contraction. Low-voltage AC injury with loss of consciousness and/or arrest In respiratory arrest or ventricular fibrillation that is not witnessed, an electrical exposure may be difficult to diagnose. All unwitnessed arrests should include this possibility in the differential diagnosis. Query EMS personnel, family, and coworkers about this possibility. Inquire if a scream was heard before the patient’s collapse; this may be due to involuntary contraction of chest wall muscles from electrical current. High-voltage AC injury without loss of consciousness and/or arrest Usually high-voltage injuries do not cause loss of consciousness but instead cause devastating thermal burns. In occupational exposures, details of voltage can be obtained from the local power company. High-voltage AC injury with loss of consciousness and/or arrest This is an unusual presentation of high-voltage AC injuries, which do not often cause loss of consciousness. History may need to come from bystanders or EMS personnel. Direct current (DC) injury These injuries typically cause a single muscle contraction that throws the victim away from the source. They are rarely associated with loss of consciousness unless there is severe head trauma, and victims can often provide their own history. Conducted electrical devices Conducted electrical weapons (CEWs) such as tasers are weapons used by law enforcement that deliver high-voltage current that is neither true AC or DC but is most like a series of low-amplitude DC shocks.[16] They can deliver 50,000 V in a 5-second pulse, with an average current of 2.1 mA.[17] Though they have been temporally associated with deaths in the law enforcement setting, conducted electrical devices (CEDs) in healthy volunteers have been shown to be safe without evidence of delayed arrhythmia or cardiac damage as measured by troponin I.[18, 17] One study of their use in 1201 law enforcement incidents showed mostly superficial puncture wounds from the device probes, and significant injuries only from trauma subsequent to shock, not from the device itself. Of 2 deaths in custody, neither was related to CEW exposure.[19]

Your stomach must be empty, so you should not eat or drink anything for approximately 8 hours before the examination. Your physician will be more specific about the time to begin fasting depending on the time of day that your test is scheduled. Your current medications may need to be adjusted or avoided. Most medications can be continued as usual. Medication use such as aspirin, Vitamin E, non-steroidal anti-inflammatories, blood thinners and insulin should be discussed with your physician prior to the examination as well as any other medication you might be taking. It is therefore best to inform your physician of any allergies to medications, iodine, or shellfish. It is essential that you alert your physician if you require antibiotics prior to undergoing dental procedures, since you may also require antibiotics prior to ERCP. Also, if you have any major diseases, such as heart or lung disease that may require special attention during the procedure, discuss this with your physician. To make the examination comfortable, you will be sedated during the procedure, and, therefore, you will need someone to drive you home afterward. Sedatives will affect your judgment and reflexes for the rest of the day, so you should not drive or operate machinery until the next day.
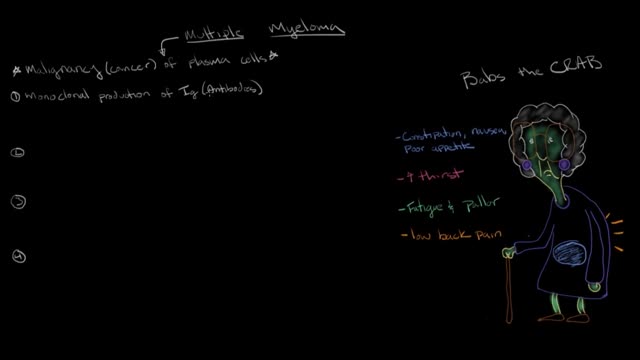
Multiple myeloma is a cancer that affects plasma cells, a kind of white blood cell found in the soft insides of your bones, called marrow. Plasma cells are part of your body's immune system. They make antibodies to help fight off infections.

The pain is frequently severe and is described as throbbing or pulsating. Nausea is common, and many migraine patients have a watering eye, a running nose, or congestion. If these symptoms are prominent, they may lead to a misdiagnosis of sinus headaches.
Addison's disease is a disorder that occurs when your body produces insufficient amounts of certain hormones produced by your adrenal glands. In Addison's disease, your adrenal glands produce too little cortisol and often insufficient levels of aldosterone as well. Also called adrenal insufficiency, Addison's disease occurs in all age groups and affects both sexes. Addison's disease can be life-threatening. Treatment for Addison's disease involves taking hormones to replace the insufficient amounts being made by your adrenal glands, in order to mimic the beneficial effects produced by your naturally made hormones.

Blunt injury to the heart ranges from contusion to disruption. This report comprises 14 patients seen during a 6-year period with cardiac rupture secondary to blunt trauma. Eight patients were injured in automobile accidents, two patients were injured in auto-pedestrian accidents, two were kicked in the chest by ungulates, and two sustained falls. Cardiac tamponade was suspected in ten patients. Five patients presented with prehospital cardiac arrest or arrested shortly after arrival. All underwent emergency department thoracotomy without survival. Two patients expired in the operating room during attempted cardiac repair; both had significant extracardiac injury. Seven patients survived, three had right atrial injuries, three had right ventricular injuries, and one had a left atrial injury. Cardiopulmonary bypass was not required for repair of the surviving patients. There were no significant complications from the cardiac repair.
7 Simple And Natural Ways To Become A Virgin Again
