- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Hardware removals are among the most commonly performed surgical procedures worldwide. Current literature offers little data concerning postoperative patient satisfaction. The purpose of our study was to evaluate the patients’ point of view on implant removal. watch to learn more.

An African traditional healer performing a brain surgery.

http://plantar-fasciitis-solution.info-pro.co Plantar Fasciitis Symptoms, Foot Pain Running, Foot Pain Ball Of Foot, Taping For Plantar Fasciitis Home Treatments. Knowing what the cause of the pain is and why the pain is occurring enables a person more effectively tackle home treatments and remedies for plantar fasciitis. Dedicated exercise rehabilitation is one home treatment technique that has been proven to address the deficiencies identified in the plantar fascia tissue. Determine the severity of the pain being experienced and this may provide an idea regarding the level of exercise the affected foot can accommodate at a time. It can be possible to use anti-inflammatory medications or natural nutritional substances that contain anti-inflammatory properties to relieve pain symptoms associated with plantar fasciitis. While gently exercising the affected foot or feet, it is important to avoid activity that can exacerbate the condition. This is why a person with plantar fasciitis can notice pain when resuming activity with the feet after being in a resting position for a period of time. Also, an important home treatment for plantar fasciitis is rest! The affected foot needs rest and this can help the healing process. If you would like more information Click HERE To Learn More About Plantar Fasciitis. http://plantar-fasciitis-solution.info-pro.co

Funny Video from hospital waiting room

TV Interview with Dr. Mostafa Yakoot, MD about the novel Influenza H1N1 (Swine Flu)
Updates in triage and management.
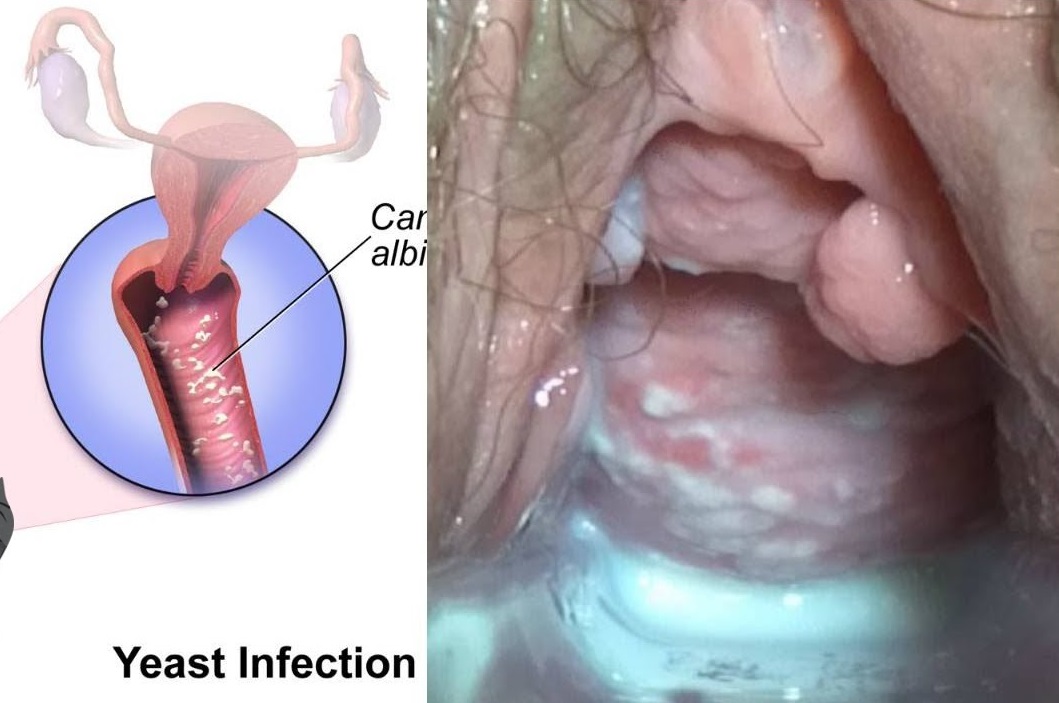
Watch that video to know Types and Causes of Vaginal Infection Yeast or Candidiasis, Trichomoniasis or Bacterial ?

A growing number of patients having total knee replacement surgery are 55 or younger. Surgeons at Sunnybrook's Holland Centre perform more than 1,000 total knee replacements each year. Read more: http://sunnyview.sunnybrook.ca..../2011/11/snap-crackl

Loyola Full Male Exam Part 4 A video from Loyola medical school, Chicago showing the full examination of the male
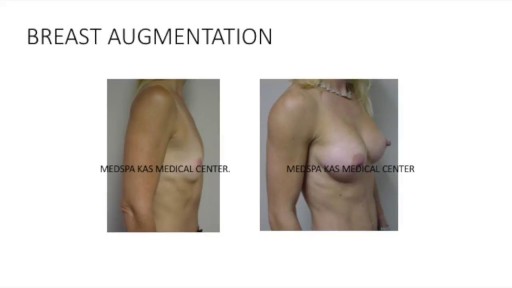
This is a complete video of breast augmentation procedure with implants also includes some before after photographs of breast augmentation surgery by Dr. Ajaya Kashyap at MedSpa Clinic, Delhi, India. source: https://www.youtube.com/watch?v=tRg3RkvCvOE Get more information: www.bestbreastsurgeryindia.com Get more information: www.themedspa.us Email at: info@themedspa.us Call/WhatsApp on:+91-9818369662, 9958221983/82/81

(cryptorchidism) is a testicle that hasn't moved into its proper position in the bag of skin hanging below the penis (scrotum) before birth. Usually just one testicle is affected, but about 10 percent of the time both testicles are undescended. An undescended testicle is uncommon in general, but common among baby boys born prematurely. The vast majority of the time, the undescended testicle moves into the proper position on its own, within the first few months of life. If your son has an undescended testicle that doesn't correct itself, surgery can relocate the testicle into the scrotum.
Watch that video to know about the Health Benefits from KISSING

28 years old gentleman presented with huge liver abscess in the right lobe, with repeated attempts of percutaneous aspirations in the past. He was evaluated and subjected to Laparoscopic drainage. This video depicts feasibility of laparoscopy in deep seated liver abscesses. Video created by: Dr. Juneed M. Lanker Fellow Minimal Access Surgery Apollo Hospitals Chennai.

It is very important to instruct your patients about how to self exam their breasts for any abnormalities or masses for early detection of any changes
Regime Rapide, Perdre De La Graisse, Rajeunissement, Corps Neuf, Exercices Pour Perdre Du Poids ---- http://rajeunir-de-10-ans.info-pro.co --- Pourquoi vous ne devriez jamais vous entraîner plus de 90 minutes par semaine Saviez-vous que vous entraîner plus de 90 minutes par semaine peut accélérer le vieillissement de votre corps plus rapidement? Cet article de mon copain Steve Holman explique exactement pourquoi: http://rajeunir-de-10-ans.info-pro.co Dans l'article, il partage également avec vous cinq techniques bizarres pour paraître dix ans plus jeune ... des choses étonnantes dont vous n'avez probablement jamais entendu parler auparavant. Vérifiez les ici: http://rajeunir-de-10-ans.info-pro.co Les dangers de TROP faire d'exercices! Dans l'article, il partage également avec vous 5 façons uniques pour paraître dix ans plus jeune ... des choses étonnantes dont vous n'avez probablement jamais entendu parler auparavant. Vérifiez- les ici: http://rajeunir-de-10-ans.info-pro.co 5 façons uniques pour paraître dix ans plus jeune (et les dangers de faire trop d'exercice) Les 5 étapes pour Rajeunir de 10 ans! Cliquez Ici: http://rajeunir-de-10-ans.info-pro.co

Watch that video of The Most Invasive Parasites in the World
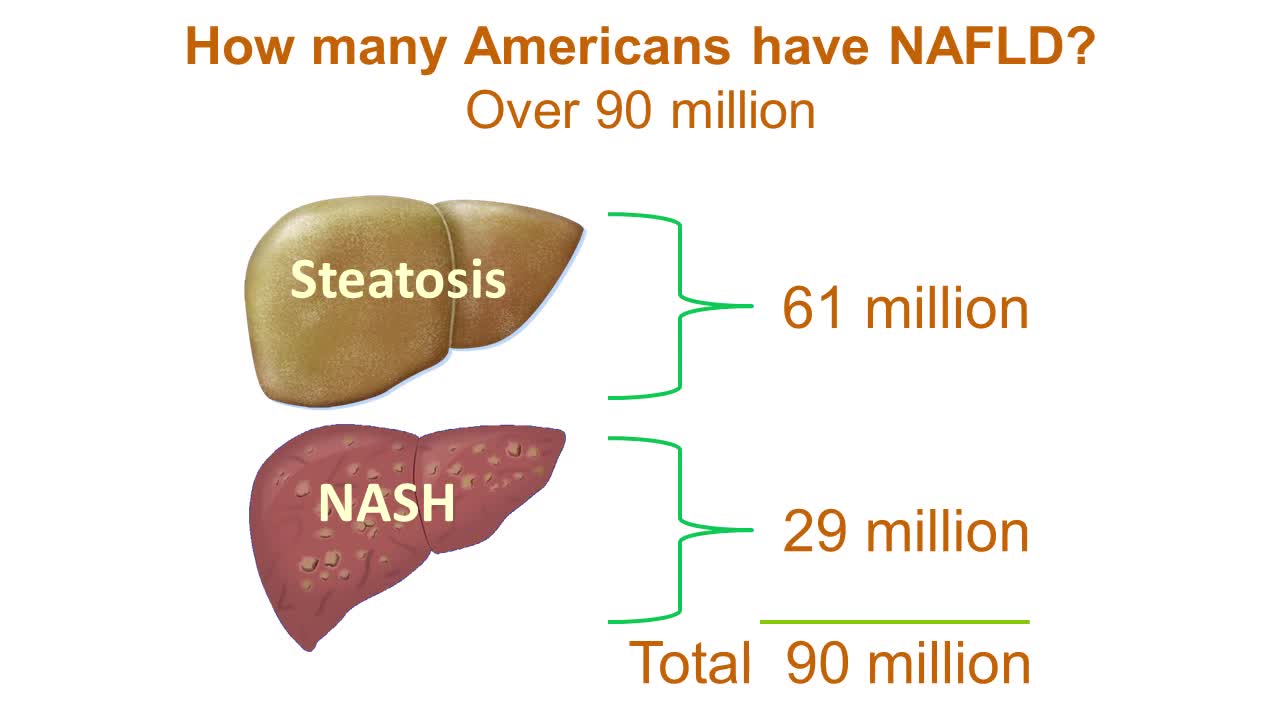
Nonalcoholic fatty liver disease is an umbrella term for a range of liver conditions affecting people who drink little to no alcohol. As the name implies, the main characteristic of nonalcoholic fatty liver disease is too much fat stored in liver cells. Nonalcoholic steatohepatitis, a potentially serious form of the disease, is marked by liver inflammation, which may progress to scarring and irreversible damage. This damage is similar to the damage caused by heavy alcohol use. At its most severe, nonalcoholic steatohepatitis can progress to cirrhosis and liver failure Nonalcoholic fatty liver disease is increasingly common around the world, especially in Western nations. In the United States, it is the most common form of chronic liver disease, affecting an estimated 80 to 100 million people. Nonalcoholic fatty liver disease occurs in every age group but especially in people in their 40s and 50s who are at high risk of heart disease because of such risk factors as obesity and type 2 diabetes. The condition is also closely linked to metabolic syndrome, which is a cluster of abnormalities including increased abdominal fat, poor ability to use the hormone insulin, high blood pressure and high blood levels of triglycerides, a type of fat. Nonalcoholic fatty liver disease care at Mayo Clinic Request an Appointment at Mayo Clinic Symptoms & causes Aug. 23, 2016 Print Share on: Facebook Twitter References Related Magnetic resonance elastography Nonalcoholic fatty liver disease Overview Symptoms & causes Diagnosis & treatment Diagnosis Treatment Departments & specialties Expertise & rankings Locations, travel & lodging Clinical trials Research Costs & insurance Preparing for your appointment Self-management More about In-Depth Multimedia Resources News from Mayo Clinic Advertisement
This medical animation shows laparoscopically assisted gallbladder removal surgery, or cholecystectomy. The animation begins by showing the normal anatomy of the liver and gallbladder. Over time, gallstones form within the gallbladder, blocking the cystic duct, and causing the gallbladder to become enlarged and inflamed. The procedure, sometimes called a "lap-chole", begins with the insertion of four trocar devices, which allow the physician to see inside the abdomen without making a large incision. Air is added to the abdominal cavity to make it easier to see the gall bladder. Next, we see a view through the laparascope, showing two surgical instruments grasping the gallbladder while a third severs the cystic duct. After the gallbladder is removed, the camera pans around to show that the cystic artery and vein, have already been clipped to prevent bleeding.
Item #ANIM026
An OB/GYN nurse from Erlanger Hospital discusses caring for a newborn baby after a circumcision.

How are seizures and epilepsy treated? What should I do if someone has a seizure? When seizure medications don't work, what else can be tried? These are just a few of the questions that you'll find answered here. Some treatment goals are common to everyone. Everyone should know what to do when a person is having a seizure. All people with seizures and their families should know that the real goal of treating epilepsy is to stop seizures or control them as best as possible. But you are more than just a seizure and how epilepsy affects you and your family may be different from someone else. Don't forget the most important goal of the Epilepsy Foundation - helping people with seizures and their families lead full and unrestricted lives according to their own wishes. Patient and doctor discussing treatment options"No seizures, no side effects" is the motto for epilepsy treatment. Not every person will reach that goal right now, but research and getting the "right care at the right time" can help more people achieve it each year. You may learn things here that can help you right away or later on. While seizure medicines are the mainstay of epilepsy treatment, there are other approaches to think about too. We hope these sections will help you learn about different treatments and get the help you need. Learn about the basics of Treatment 101 to help you get started. Look at Receiving Quality Care to see what to expect when you have just been diagnosed or after you have already started treatment. Then learn about specific treatments, what to do if seizures don't stop, and how to develop your health care team. You'll also find tools to help you manage your epilepsy or learn about research studies in other sections, so don't stop here!

Sean Langenfeld, M.D., UNMC College of Medicine
