- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
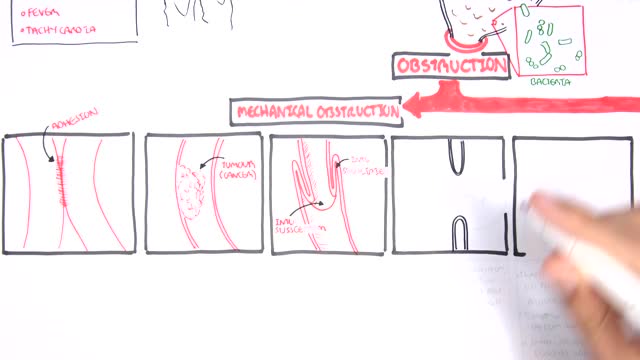
A small-bowel obstruction (SBO) is caused by a variety of pathologic processes. The leading cause of SBO in industrialized countries is postoperative adhesions (60%), followed by malignancy, Crohn disease, and hernias, although some studies have reported Crohn disease as a greater etiologic factor than neoplasia.

Experts do not know the exact cause of Zollinger-Ellison syndrome. About 25 to 30 percent of gastrinomas are caused by an inherited genetic disorder called multiple endocrine neoplasia type 1 (MEN1). MEN1 causes hormone-releasing tumors in the endocrine glands and the duodenum.
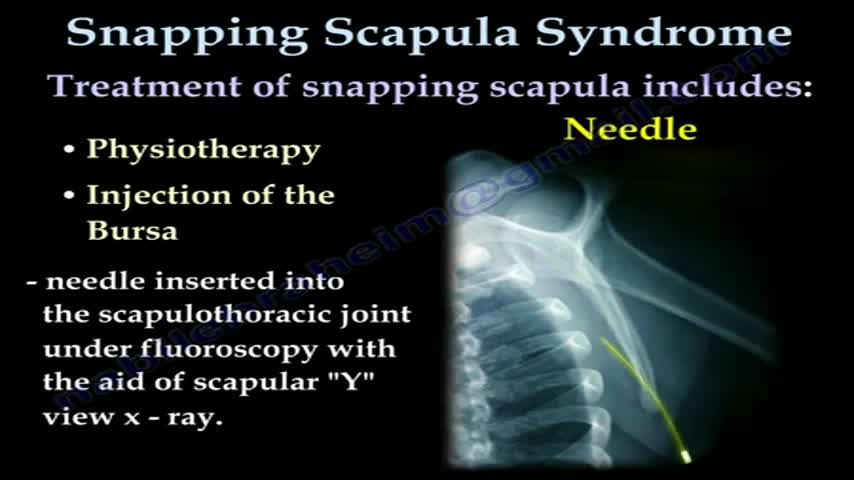
... Orthopedics & Sports Medicine Our Services Where Does it Hurt? SNAPPING SCAPULA SYNDROME PDF Icon PRINTABLE BOOKLET A PATIENT'S GUIDE TO SNAPPING SCAPULA SYNDROME INTRODUCTION The scapulothoracic joint is located where the shoulder blade (also called the scapula) glides along the chest wall (the thorax). When movement of this joint causes feelings or sounds of grating, grinding, popping, or thumping, doctors call it snapping scapula syndrome. Snapping scapula syndrome is fairly rare. When it happens, the soft tissues between the scapula and the chest wall are thick, irritated, or inflamed. Snapping scapula syndrome can also happen if the bones of the shoulder blade or rib cage grate over one another. This guide will help you understand what causes snapping scapula syndrome how doctors treat this condition ANATOMY What parts of the body are involved in this condition? The shoulder is made up of three bones: the humerus (upper arm bone), the clavicle (collarbone), and the scapula(shoulder blade). Two large muscles attach to the front part of the scapula where it rests against the chest wall. One of them, called the subscapularis muscle, attaches over the front of the scapula where it faces the chest wall. The serratus anterior muscle attaches along the edge of the scapula nearest the spine. It passes in front of the scapula, wraps around the chest wall, and connects to the ribs on the front part of the chest. A bursa is a fluid-filled sac that cushions body tissues from friction. A bursa sits between the two muscles of the scapula. There is also a bursa in the space between the serratus anterior muscle and the chest wall. When bursa sacs become inflamed, the condition is called bursitis. Scapulothoracic bursitis refers to inflammation in the bursa under the shoulder blade. This type of bursitis is most common in the upper corner of the scapula nearest the spine. It also occurs under the lower tip of the scapula. In either case, it can cause the sounds and sensations of snapping scapula syndrome. A person can have bursitis in the joint without any grinding or popping. Related Document: A Patient's Guide to Shoulder Anatomy CAUSES What causes this condition? Snapping scapula is caused by problems in the soft tissues or bones of the scapula and chest wall. It can start when the tissues between the scapula and shoulder blade thicken from inflammation. The inflammation is usually caused by repetitive movements. Certain motions of the shoulder done over and over again, such as the movements of pitching baseballs or hanging wallpaper, can cause the tissues of the joint to become inflamed. In other cases, the muscles under the scapula have shrunk (atrophied) from weakness or inactivity. The scapula bone then rides more closely to the rib cage. This means the scapula bumps or rubs on the rib bones during movement. Changes in the alignment or contour of the bones of the scapulothoracic joint can also cause snapping scapula. When a fractured rib or scapula isn't lined up just right, it can cause a bumpy ridge that produces the characteristic grind or snap as the scapula moves over the chest wall.
These air sacs make up most of the lung tissue. Lung diseases affecting the alveoli include: Pneumonia: An infection of the alveoli, usually by bacteria. Tuberculosis: A slowly progressive pneumonia caused by the bacteria Mycobacterium tuberculosis. Chronic respiratory diseases are chronic diseases of the airways and other structures of the lung. Some of the most common are: asthma, chronic obstructive pulmonary disease, occupational lung diseases and pulmonary hypertension.
If you’re considering an epidural to help manage the pain of childbirth, you’re not alone. More than 60 percent of women delivering at hospitals elect for an epidural during labor. And with good reason: An epidural is considered one of the safest methods of pain control, with just one in 3,000 pregnancies experiencing serious complications. It’s also good for you, since you’ll remain awake and alert during the birth, as well as for your baby, since the drugs will barely reach your bloodstream (so they can’t get into hers).
Is Air Travel During Pregnancy Safe? Traveling by air is considered safe for women while they are pregnant; however, the following ideas might make your trip safer and more comfortable. Most airlines allow pregnant women to travel through their eighth month.

For strong lungs, chew 3 to 5 peppermint leaves each day. To treat congestion, add a few drops of peppermint oil to a pot of hot water and inhale the steam. You can also drink 2 cups of peppermint tea daily. To make the tea, add 1 teaspoon of dried peppermint leaves to a cup of hot water.

Spina bifida is a condition that affects the spine and is usually apparent at birth. It is a type of neural tube defect (NTD). Spina bifida can happen anywhere along the spine if the neural tube does not close all the way. When the neural tube doesn’t close all the way, the backbone that protects the spinal cord doesn’t form and close as it should. This often results in damage to the spinal cord and nerves. Spina bifida might cause physical and intellectual disabilities that range from mild to severe. The severity depends on: The size and location of the opening in the spine. Whether part of the spinal cord and nerves are affected.
The first transplant of a bionic eye on a patient with a rare disease.

Periods are considered to be one of the most taboo topics to talk about, but they can reveal a plethora of information when it comes to your health. Whether you last publicly learned about menstruation in fifth grade or during a junior high school sex ed class, it’s time to unravel what Aunt Flo and your hormonal health have to do with one another. Look before you flush not only when it comes to your urine or poop, but also your period, and find out the six things your monthly visitor can tell you about your health from what’s normal to what’s not at any age.

Face transplant allows this man to live a normal life. Hats off to all the surgeons involved!
This technique could solve the organ shortage crisis.

Vaccination is now mandatory in Italy.

The first operation is harvesting the heart from the donor. The donor is usually an unfortunate person who has suffered irreversible brain injury, called "brain death". Very often these are patients who have had major trauma to the head, for example, in an automobile accident. The victim's organs, other than the brain, are working well with the help of medications and other "life support" that may include a respirator or other devices. A team of physicians, nurses, and technicians goes to the hospital of the donor to remove donated organs once brain death of the donor has been determined. The removed organs are transported on ice to keep them alive until they can be implanted. For the heart, this is optimally less than six hours. So, the organs are often flown by airplane or helicopter to the recipient's hospital.

The first week after birth: What to expect

New-born baby having a bath
30 yr old man presented to ER after Motor Vehicle Crash..blunt chest trauma...

In this video, I will be sharing simple tests and exercises which will diagnose your knee pain.
These tests will help with the knee pain diagnosis.
In addition, I will share the most effective therapy and exercises with you which you can do from the comfort of your own home.
Time Stamp:
00:00 Introduction
00:59 Anatomy Inside of the Knee
02:19 Test for Pain on Inside of knee (MCL)
03:12 HARM Protocol
03:30 POLICE Protocol
04:44 Home Therapy MCL Sprain
06:06 Home Exercises MCL Sprain
09:21 Test for Pain on Outside of Knee (LCL)
11:11 Renne's Test (ITB Band)
13:39 Symptoms of Meniscus Tear
13:59 Thessaly Test for Meniscus Tear
14:49 Ege's Test for Meniscus Tear
Our Clinics:
Milton Chiropractic Clinic
2 Ely Road
Milton, Cambridge
CB24 6DD
United Kingdom
Tel: +44 (0) 1223 864444
https://www.miltonchiropractic.co.uk
Fornham Chiropractic Clinic
Unit 10
Fornham Business Court
Hall Farm
Fornham St Martin
Bury St Edmunds
IP31 1SL
United Kingdom
Tel: +44 (0) 1284 220202
https://www.fornhamchiropractic.co.uk

In this video, the 1st Breast Reduction Surgery had been performed 10 years ago which had resulted in asymmetry. In this breast reduction surgery the breast asymmetry was corrected and the large size of both areolas was addressed.
