- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Stop suffering alone and get relief from vaginal atrophy symptoms

Twin Childbirth Video

Human immunodeficiency virus infection / acquired immunodeficiency syndrome (HIV/AIDS) is a disease of the human immune system caused by the human immunodeficiency virus (HIV).[1] During the initial infection a person may experience a brief period of influenza-like illness. This is typically followed by a prolonged period without symptoms. As the illness progresses it interferes more and more with the immune system, making people much more likely to get infections, including opportunistic infections, and tumors that do not usually affect people with working immune systems.
HIV is transmitted primarily via unprotected sexual intercourse (including anal and even oral sex), contaminated blood transfusions and hypodermic needles, and from mother to child during pregnancy, delivery, or breastfeeding.[2] Some bodily fluids, such as saliva and tears, do not transmit HIV.[3] Prevention of HIV infection, primarily through safe sex and needle-exchange programs, is a key strategy to control the spread of the disease. There is no cure or vaccine; however, antiretroviral treatment can slow the course of the disease and may lead to a near-normal life expectancy. While antiretroviral treatment reduces the risk of death and complications from the disease, these medications are expensive and may be associated with side effects.
Genetic research indicates that HIV originated in West-central Africa during the early twentieth century.[4] AIDS was first recognized by the Centers for Disease Control and Prevention (CDC) in 1981 and its cause—HIV infection—was identified in the early part of the decade.[5] Since its discovery, AIDS has caused nearly 30 million deaths (as of 2009).[6] As of 2010, approximately 34 million people have contracted HIV globally.[7] AIDS is considered a pandemic—a disease outbreak which is present over a large area and is actively spreading.[8]
HIV/AIDS has had a great impact on society, both as an illness and as a source of discrimination. The disease also has significant economic impacts. There are many misconceptions about HIV/AIDS such as the belief that it can be transmitted by casual non-sexual contact. The disease has also become subject to many controversies involving religion.
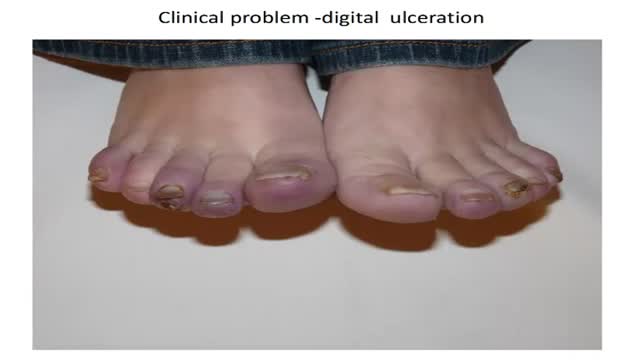
How to diagnose digital ulceration in out patient clinic.
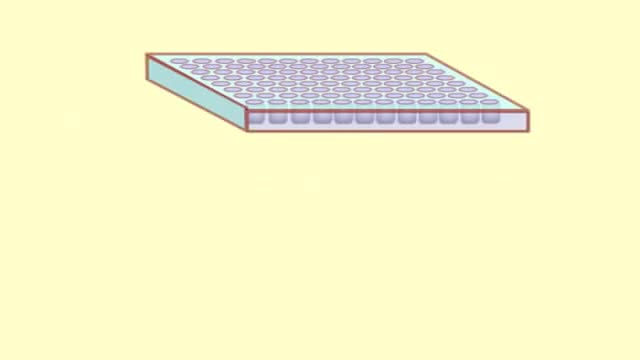
The purpose of an ELISA is to determine if a particular protein is present in a sample and if so, how much. There are two main variations on this method: you can determine how much antibody is in a sample, or you can determine how much protein is bound by an antibody. The distinction is whether you are trying to quantify an antibody or some other protein. In this example, we will use an ELISA to determine how much of a particular antibody is present in an individuals blood.
ELISAs are performed in 96-well plates which permits high throughput results. The bottom of each well is coated with a protein to which will bind the antibody you want to measure. Whole blood is allowed to clot and the cells are centrifuged out to obtain the clear serum with antibodies (called primary antibodies). The serum is incubated in a well, and each well contains a different serum (see figure below). A positive control serum and a negative control serum would be included among the 96 samples being tested.

This video shows the delivery of the placenta after delivery of the fetus

Whether you need to boost your energy or curb an afternoon craving, staying hydrated is made easy with these tips.

Holoprosencephally

http://segreti-per-dimagrire.plus101.com
---Camminare Fa Dimagrire. Ho sempre lottato con il mio peso. Ho sempre provato un programma di dimagrimento per qualche mese ma poi niente, non ho mai perso più di 2-3 kg. Vi posso assicurare che il programma Formula per dimagrire mi ha cambiato la vita. I miei amici e parenti mi chiedono continuamente come ho fatto..non potrei essere più felice di ora, quando mi guardo allo specchio vedo un'altra persona Mirko Calì
http://www.youtube.com/watch?v=qPmqxvzwyTs
Camminare Fa Dimagrire
http://www.youtube.com/user/DietaPanciaPiatta
http://www.youtube.com/user/DietaSettimanale
http://www.youtube.com/user/MetodiPerDimagrire1
http://www.youtube.com/user/ComePossoDimagrire
Camminare Fa Dimagrire,
come si dimagrisce velocemente,
come si fa dimagrire,
come si fa dimagrire in fretta,
come si puo dimagrire,
compresse dimagranti,
compresse per dimagrire,
consigli alimentari per dimagrire,
consigli alimentari per perdere peso,
consigli come dimagrire,
consigli del nutrizionista per perdere peso,
consigli dimagrire,
consigli dimagrire velocemente,
consigli per dieta,
consigli per dimagrire,
consigli per dimagrire senza dieta,

http://vaincre-le-diabete.plus101.com
---Traitement Diabete 2. Vous Eliminerez Le Diabète D'Une Fois Pour Toutes!
Laissez de côté les préoccupations des risques de votre maladie.
Ne souffrez plus de votre poids et la privation des aliments préférés.
Ne dépensez plus des milliers d'euros en médicaments qui combattent la maladie de l'extérieur.
Ne vivez plus une vie de restrictions.
Ne souffrez plus!!!
Oubliez de changer constamment de médicaments prescrits, de mesurer le niveau de glucose et de vous injecter l'insuline.
Traitement Diabete 2
http://youtu.be/SvsCAZuKGBo
traitement contre le diabete de type 2,
traitement de diabete type 2,
traitement de diabète de type 2,
traitement diabete type 1,
traitement diabète de type 2,
traitement diabète type 2,
traitement du diabete type 2 par les plantes,
traitement du diabète de type 2,
traitement du diabète par les plantes,
traitement du diabète type 2,
traitement naturel diabete,
traitement pour diabete,
traitement pour le diabète de type 2,
traitements diabète
Pomada Para Herpes, Como Curar Herpes, Imagenes De Herpes Labial, Como Curar Un Herpes.
http://como-curar-el-herpes.good-info.co
Y aquí hay un hecho que probablemente no sabías:
No hay mucha diferencia con el herpes..
Si lo cubres con fármacos supresores todavía socavas tu salud.
Incluso te puede matar por abrir las puertas para un ejército de otras enfermedades. Por ejemplo...
Tienes de 2 a 4 veces más probabilidades de contraer HIV de acuerdo a la Universidad de Washintong
¿Y qué pasa con las convulsiones e hinchazón del tejido de tu cerebro, que de tan malo puede hacer estallar tu cráneo?
Lo que suena como el guión de una película de terror se llama "meningitis". Mata al 11% de sus víctimas
Para mas información
http://como-curar-el-herpes.good-info.co
Suscríbete A nuestro Canal
https://www.youtube.com/watch?v=4qxFM-3kF8k
Visita Nuestro Blog
http://que-es-el-herpes.blogspot.com/
Pomada Para Herpes, Como Curar Herpes, Imagenes De Herpes Labial, Como Curar Un Herpes, causas herpes simple, fotos herpes labial, como es el herpes en la piel, como curar un herpes en la boca, forma de contagio del herpes, tratamiento natural para el herpes, herpes labial medicina, herpes bucal causas, tratamiento del herpes bucal, como curar un herpes, herpes oral causas, herpes tratamiento medico, herpes viral tratamiento, herpes boca causas, tratamiento del herpes zoster

Insulina, Sintomi Iperglicemia, Dolci Per Diabetici Ricette, Giornata Mondiale Del Diabete
http://diabete-cura.info-pro.co
Abbassa il livello di zucchero nel sangue e liberati dall’insulina in tre settimane o meno ... GARANTITO!
Ogni giorno, negli Stati Uniti, vengono diagnosticati più di 2000 nuovi casi di diabete.
Con l'attenzione focalizzata sui livelli di zucchero nel sangue e insulina, tuttavia, la causa di tutta la devastazione è stata trascurata.
Questo ebook rivoluzionario rivela la causa principale del diabete e come invertire il processo.
Il diabete è una malattia che se non si prende un'azione efficace contro di essa, peggiora sempre di più.
Purtroppo, i farmaci curano solo i sintomi del diabete e di solito non fanno nulla per affrontare le cause sottostanti.
PER COMINCIARE A GUARIRE DAL DIABETE
come curare il diabete in modo naturale e garantito senza farmaci e insulina! CLICCA QUI: http://diabete-cura.info-pro.co
Clicca sul link sottostante per fare il check out
http://diabete-cura.info-pro.co
Iscriviti al nostro canale
http://www.youtube.com/user/viveresano01
https://www.youtube.com/watch?v=1sul1papqgk
Insulina, Sintomi Iperglicemia, Dolci Per Diabetici Ricette, Giornata Mondiale Del Diabete,
diabete mellito,
sintomi diabete,
diabete sintomi,
diabete tipo 2,
dieta per diabetici,
diabete insipido,
diabete gestazionale,
diabete tipo 1,
dolci per diabetici,
sintomi del diabete,
iperglicemia,
diabete mellito tipo 2,
dieta diabete
How we went from super species to the sickest. What gravity has to do with it.
Neuropathic pain: often difficult to treat. Palmitoylethanolamide (PEA) is a very special molecule, produced in our own body, against pain and chronic inflammation. PEA is available as supplement and as cream, and as dietfood for medical purposes in Italy and Spain. It has been explored since 1957 and has a clear analgesic and anti-inflammatory efficacy, and virtually no side effects. Meanwhile within the context of clinical trials 5000 patients have been using PEA, and its efficacy and safety has been documented in more than 400 scientific papers: http://palmitoylethanolamide4pain.com/about-2/ a website containing 400+ scientific articles on PEA in 6 different languages. The PEA datapool.

Vaser is additionally called as Ultrasonic Assisted Lipoplasty. The 4 th era vaser has exceptional plan and capacities. The test has single or various rings to appropriate the ultrasonic vitality radially emulsifying the fat consistently. Less the quantity of rings more power is produced at the tip which is valuable for intense fibrofatty tissue or remedial surgery.
see details here : http://vaser-dubai.com

Dr. David Salvador provides ultrasonic liposuction for removing fat in West Palm Beach FL.

Best facial cosmetic surgeons Best facial plastic surgeon Browlift Charlotte endoscopic brow lift Charlotte’s top facial plastic surgeon Facial plastic surgeons Facial plastic surgery Face lifts Facial mini-tuck Lip enhancement Lip augmentation Nose job Nose job cost Nose surgery Rhinoplasty Rhinoplasty Expert Rhinoplasty and teens Revision rhinoplasty Teen Rhinoplasty, Charlotte Teen Rhinoplasty, North Carolina Teen Rhinoplasty Expert Top rhinoplasty surgeons Best Charlotte rhinoplasty surgeons:

Best facial cosmetic surgeons Best facial plastic surgeon Browlift Charlotte endoscopic brow lift Charlotte’s top facial plastic surgeon Facial plastic surgeons Facial plastic surgery Face lifts Facial mini-tuck Lip enhancement Lip augmentation Nose job Nose job cost Nose surgery Rhinoplasty Rhinoplasty Expert Rhinoplasty and teens Revision rhinoplasty Teen Rhinoplasty, Charlotte Teen Rhinoplasty, North Carolina Teen Rhinoplasty Expert Top rhinoplasty surgeons Best Charlotte rhinoplasty surgeons: C local listings,#8, 9 organic listings Most experienced rhinoplasty surgeons

Best and 100% Successful Hymen Repair Surgery in Delhi with Latest Ultrafine Hymen repair Technology. 100% successful , Secure and Private. for more information visit: http://www.olmeccosmeticsurgery.com/best-hymenoplasty-surgery-india-delhi/

Skin Cysts Cysts are noncancerous, closed pockets of tissue that can be filled with fluid, pus, or other material. Cysts are common on the skin and can appear anywhere. They feel like large peas under the surface of the skin. Cysts can develop as a result of infection, clogging of sebaceous glands (oil glands), or around foreign bodies, such as earrings.
