- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Heart Attack Angioplasty Procedure Animation Video

Preparing The Kidney for Transplant


It demonstrates basic suturing techniques as might be applied in an emergency room setting.
Arterial Blood Gas Sampling
The Ex-PRESS Mini Glaucoma Shunt provides a simplified method of filtration surgery for patients with open angle glaucoma. The Ex-PRESS implanted Under a Scleral Flap is a minimally invasive procedure with predictable results.

Clamping the umbilical cord and assessment of the apgar score of the baby

Michael Marcus, MD Pediatric Pulmonary www.DrMDK.com Maimonides Medical Center Fellowship:Children’s Hospital of Philadelphia www.DrMDK.com

Examination of the heart from the USMLE collection

A video showing Cystocele Repair
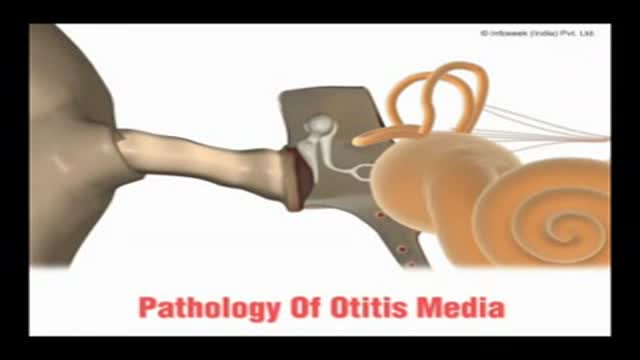
A video showing the pathology of otitis media

تناسق القوام مطلب كل أنسان سواء رجل أو أمرأة ولذلك يجب تحديد معدل تراكم الدهون بالجسم و تحديد نوع تناسق القوام و كيفيته
د. محمد الروبي
استشارى جراحات التجميل بجامعة عين شمس

Breast reduction can relieve strain from shoulder straps, neck, back, and upper arms.
It can provide an uplift to help clothes fit and look better. Traditionally, insurance companies would provide benefits for a broad range of breast sizes and gram weight of tissue to be removed from each breast. At present most insurance companies limit authorization when the doctor plans to remove less than 500gm weight per breast. Since many patients present with symptoms in a D cup to DD cup, often, the very removal of over 500 grams weight may reduce the breasts too much. This amount of reduction may not be in harmony with body shape. Newer methods of breast assembly after reduction, will tighten things using internal brassiere techniques that also compact and reduce breast volume. Therefore, a gram weight reduction of 500gms in some patients combined with internal tightening efforts, could pose an over-reduction. With the unreliability of insurance support in some cases, it is best not to look solely at gram weight in the surgical planning of breast reduction. When excess skin and weight is removed, the improved location of the breasts on the chest will give marked relief of symptoms.
Surgery takes from 2 to 5 hours and can be done as an outpatient or with a brief overnight stay. When possible, no scarring other than around the areola can be planned which follows the Brazilian and French methods (Goes and Benelli). For very large reductions, a vertical method, or T pattern approach is offered. Recovery is a few days, with special care to avoid strain for 4 to 6 weeks. Some soreness may persist for a few weeks. The breasts can appear tight, swollen, and bruised at first, but will usually settle to their near final look by 6 weeks. There may be sutures to be removed in some cases. Costs relate to the severity of the sag, and weight of the breasts.
The operation can make a stunning change in body image, relief of upper body symptoms, and offer a cosmetic lift to naturally sloping breasts.

Loyola Respiratory System Exam Part 2 A video from Loyola Medical School, Chicago showing the medical and clinical examination of the respiratory system.
Technique for Popliteal/Peroneal Nerve Block
Off-Pump CABG in Dextrocardia; A New Challenge for a New Era
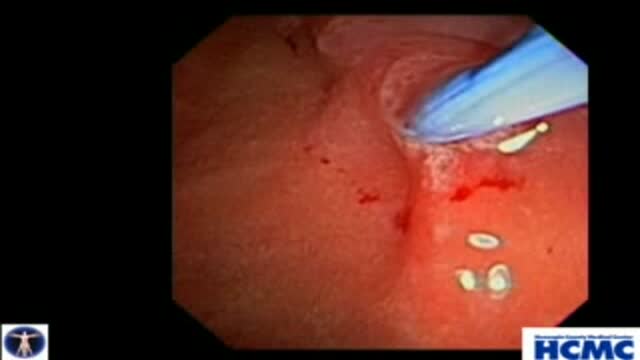
Biliary and Pancreatic Sphincterotomies for Sphincter of Oddi Dysfunction
This 43 year old woman has severe recurrent RUQ pain post cholecystectomy. Liver and pancreatic chemistries and duct size are normal, but pancreatic manometry is abnormal. The plan is to perform dual biliary and pancreatic sphincterotomy. The pancreatic duct is cannulated with a 3.9 French tip tr...iple lumen papillotome loaded with a 0.025 inch Jagwire. Contrast is injected to outline the course of the duct. The wire is passed to the tail. Notice the knuckling of the wire into the tail. This provides a safety loop, but is only safe in a small duct with use of a smaller caliber wire. Then with the wire securely in PD, papillotome is used to cannulate the bile duct. Placement of the wire in PD guarantees access for pancreatic stent placement, which is mandatory in these patients to reduce risk, it also facilitates difficult biliary cannulation. Here is the fluoroscopic view as the papillotome is passed deep into bile duct. This shows wires in the CBD and PD. Now a biliary sphincterotomy is performed, with the pancreatic guidewire in place beside the papillotome. The scope is pushed into a longer position to orient up the middle of the papilla. The sphincterotomy is done in very careful stepwise fashion to avoid perforation. Now the biliary wire is removed and the papillotome passed over the pancreatic wire for pancreatic sphincterotomy. The incision is aimed back up towards the biliary sphincterotomy to ensure the septum only is cut. Note the large pancreatic orifice. Last, a 4 French 9cm unflanged soft material pancreatic stent is placed. We always use single pigtail design to avoid inward migration of the stent. The long unflanged design allows spontaneous passage within a few weeks.

Laparoscopic Roux-en-Y Gastric Bypass Operation

Porcelain Veneers

cardiac catheterization in the work up of heart disease.
