- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A burn is tissue damage that results from scalding, overexposure to the sun or other radiation, contact with flames, chemicals or electricity, or smoke inhalation. Is it a major or minor burn? Call 911 or seek immediate care for major burns, which: Are deep Cause the skin to be dry and leathery May appear charred or have patches of white, brown or black Are larger than 3 inches (about 8 centimeters) in diameter or cover the hands, feet, face, groin, buttocks or a major joint A minor burn that doesn't require emergency care may involve: Superficial redness similar to a sunburn Pain Blisters An area no larger than 3 inches (about 8 centimeters) in diameter Treating major burns Until emergency help arrives: Protect the burned person from further harm. If you can do so safely, make sure the person you're helping is not in contact with the source of the burn. For electrical burns, make sure the power source is off before you approach the burned person. Make certain that the person burned is breathing. If needed, begin rescue breathing if you know how. Remove jewelry, belts and other restrictive items, especially from around burned areas and the neck. Burned areas swell rapidly. Cover the area of the burn. Use a cool, moist bandage or a clean cloth. Don't immerse large severe burns in water. Doing so could cause a serious loss of body heat (hypothermia). Elevate the burned area. Raise the wound above heart level, if possible. Watch for signs of shock. Signs and symptoms include fainting, pale complexion or breathing in a notably shallow fashion. Treating minor burns For minor burns: Cool the burn. Hold the burned area under cool (not cold) running water or apply a cool, wet compress until the pain eases. Remove rings or other tight items from the burned area. Try to do this quickly and gently, before the area swells. Don't break blisters. Fluid-filled blisters protect against infection. If a blister breaks, clean the area with water (mild soap is optional). Apply an antibiotic ointment. But if a rash appears, stop using the ointment. Apply lotion. Once a burn is completely cooled, apply a lotion, such as one that contains aloe vera or a moisturizer. This helps prevent drying and provides relief. Bandage the burn. Cover the burn with a sterile gauze bandage (not fluffy cotton). Wrap it loosely to avoid putting pressure on burned skin. Bandaging keeps air off the area, reduces pain and protects blistered skin. If needed, take an over-the-counter pain reliever, such as ibuprofen (Advil, Motrin IB, others), naproxen sodium (Aleve) or acetaminophen (Tylenol, others).

wound clean from pus
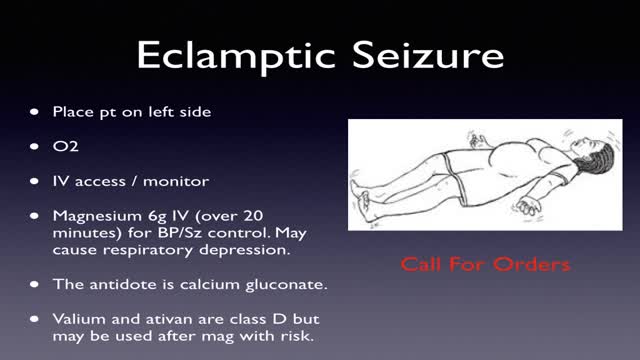
Obstetrical emergencies of pregnancy ECTOPIC PREGNANCY. ... PLACENTAL ABRUPTION. ... PLACENTA PREVIA. ... ECTOPIC PREGNANCY. ... PLACENTAL ABRUPTION. ... PLACENTA PREVIA. ... Amniotic fluid — The liquid in the placental sac that cushions the fetus and regulates temperature in the placental environment.
Trisomy 18, also called Edwards syndrome, is a chromosomal condition associated with abnormalities in many parts of the body. Individuals with trisomy 18 often have slow growth before birth (intrauterine growth retardation) and a low birth weight. Affected individuals may have heart defects and abnormalities of other organs that develop before birth. Other features of trisomy 18 include a small, abnormally shaped head; a small jaw and mouth; and clenched fists with overlapping fingers. Due to the presence of several life-threatening medical problems, many individuals with trisomy 18 die before birth or within their first month. Five to 10 percent of children with this condition live past their first year, and these children often have severe intellectual disability.
What Your Handwriting Says About You
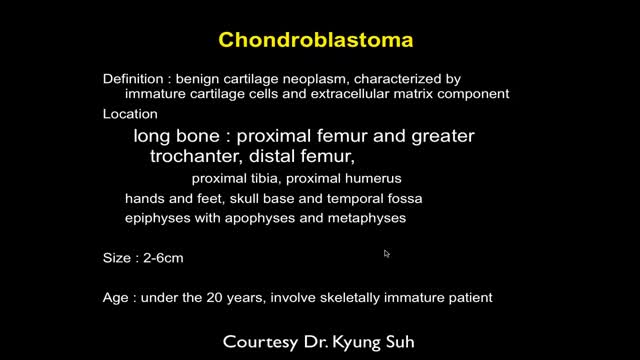
MRI of Bone Tumor
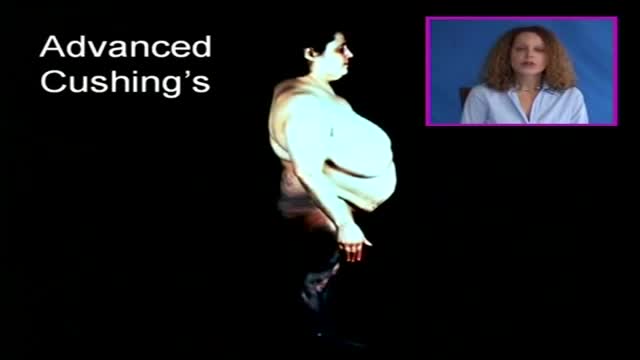
Cushing's disease is a serious condition of an excess of the steroid hormone cortisol in the blood level caused by a pituitary tumor secreting adrenocorticotropic hormone (ACTH). ACTH is a hormone produced by the normal pituitary gland. ACTH stimulates the adrenal glands (located on top of the kidneys) to produce cortisol, commonly referred to as the stress hormone.

Gastroparesis -- literally “paralyzed stomach” -- is a serious condition manifested by delayed emptying of stomach contents into the small intestine after a meal. There is no cure for gastroparesis, but treatment can speed gastric emptying and relieve gastrointestinal symptoms such as nausea and vomiting.

See the effects of cannabis first hand, unedited, on Parkinson's tremor dyskinesia, and voice.
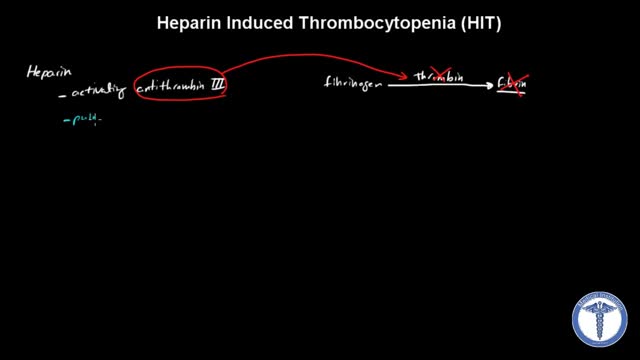
All forms of heparin (including low-molecular-weight heparin such as enoxaparin) must be stopped immediately in patients with suspected heparin-induced thrombocytopenia (HIT) while awaiting diagnostic confirmation. Patients with HIT remain at high risk of thrombosis even after discontinuation of heparin. Therefore, an alternate, rapidly acting, non-heparin anticoagulant such as direct thrombin inhibitor (eg, argatroban, bivalirudin) must be started immediately.
http://eliminar-celulite.plus101.com --- Eliminar Celulite, O Que Fazer Para Acabar Com A Celulite, Como Tirar Celulite Das Pernas. Mas as razões que vou compartilhar são diferentes das que a maioria das outras fontes está tentando fazê-la acreditar. Há um mito fazendo com que algumas mulheres acreditem que certos alimentos e nutrientes irão “eliminar as toxinas que estão causando a celulite”. ISSO É TOTALMENTE FALSO, porque não há toxinas em ou sob sua pele. Se houvesse toxinas se acumulando e ficando presas sob sua pele, você estaria morta. Simples assim. Nosso corpo foi feito para remover toxinas com muita eficácia. Este processo fisiológico acontece 24 horas por dia, 7 dias por semana, sem parar, o tempo todo. Então, a ideia não comprovada de que “toxinas” são a causa de sua celulite significa que a celulite não pode ser revertida ao “eliminá-las” com alguns alimentos, porque elas não estão lá, para começar. Mas não se preocupe, porque eis o que o planejamento alimentar apropriado pode fazer para reverter, ou prevenir, a raiz da causa da celulite em suas pernas, bumbum, quadris e coxas. Uma verdadeira dieta contra a celulite fornece nutrientes em quantidades que impactam positivamente a regulagem e equilíbrio dos hormônios femininos. Esta é a razão principal de o Planejamento Alimentar/Dieta Contra Celulite do "Adeus Celulite" só estar disponível para mulheres que começam com o Método de Exercícios SYMULAST do programa Adeus Celulite. Então se você estiver interessada, vá para: http://eliminar-celulite.plus101.com
Primary spontaneous pneumothorax is an abnormal accumulation of air in the space between the lungs and the chest cavity (called the pleural space) that can result in the partial or complete collapse of a lung. This type of pneumothorax is described as primary because it occurs in the absence of lung disease such as emphysema. Spontaneous means the pneumothorax was not caused by an injury such as a rib fracture. Primary spontaneous pneumothorax is likely due to the formation of small sacs of air (blebs) in lung tissue that rupture, causing air to leak into the pleural space. Air in the pleural space creates pressure on the lung and can lead to its collapse. A person with this condition may feel chest pain on the side of the collapsed lung and shortness of breath.

This is the future of medicine

Compromise of the blood supply from microvascular disease, often in association with lack of sensation because of neuropathy, predisposes persons with diabetes mellitus to foot infections. These infections span the spectrum from simple, superficial cellulitis to chronic osteomyelitis. Diabetic foot infections typically take one of the following forms: Cellulitis Deep-skin and soft-tissue infections Acute osteomyelitis Chronic osteomyelitis Cellulitis Tender, erythematous, nonraised skin lesions are present, sometimes with lymphangitis Lymphangitis suggests group A streptococcal infection Bullae are typical of Staphylococcus aureus infection, but occasionally occur with group A streptococci

The definition of DDH is not universally agreed upon. Typically, the term DDH is used in referring to patients who are born with dislocation or instability of the hip, which may then result in hip dysplasia. More broadly, DDH may be defined simply as abnormal growth of the hip. Abnormal development of the hip includes the osseous structures, such as the acetabulum and the proximal femur, as well as the labrum, capsule, and other soft tissues. This condition may occur at any time, from conception to skeletal maturity. The author prefers to use the term hip dysplasia, considering it both simpler and more accurate. Internationally, this disorder is still referred to as congenital dislocation of the hip.

- elbow dislocations in children are a relatively uncommon; - peak incidence occurs in adolescence between 11-15 years. - posterior dislocations are most common type; - posterior dislocation usually results from fall on outstretched hand w/ forarm supinated & elbow extended or partially flexed; - coronoid process, which nl resists posterior displacement of ulna, is relatively small in children; - anterior capsule of elbow joint is torn by force of the impact transmitted upward thru the ulna and radius

watch that video of Pulling out 1 foot long foot of gauze out from face

Fast Lower Back Pain & Sciatica Pain Relief – Beginners Yoga Stretches and Poses

Throughout your life, your skin will change constantly, for better or worse. In fact, your skin will regenerate itself approximately every 27 days. Proper skin care is essential to maintaining the health and vitality of this protective organ.