- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Dr. Rutledge and Dr. Berendes talk about severe infections seen in patients going to other countries to get less expensive surgical procedures.

Soft simple painless surgical repair of umbilical hernia video

FULL Shoulder Exam by University of Winsconsin
The video will describe the process of metabolism. Please see disclaime on my website www.academyofprofessionals.com

A 3D animation showing the diaphragm demonstrating mecanics of respiration

After 11 years of my work on my new migraine surgery, I start to do migraine surgery in all 4 principal places - places # 1 (STA) both sides, and places # 3 - Occipital artery also from both sides. You can see my first patients; he had bifrontal migraine headaches and daily chronic headaches in occipital area and the top of the head. On 30 September I sutured the occipital artery from both sides, and on 2 October I sutured STA in places # 1 from both sides. www.alisultaneh.8m.com

Just because you have asthma doesn’t mean you have to give up your daily work-out! Keep watching to amp up your exercise routine.

Recurrent varicose veins are a common problem. The patient in this video was operated for great saphenous vein insufficiency and a “neocrosse” occurred after few years. Surgical exploration revealed a “cavernoma” just over the nodes of the crural area, feeding varicose veins of thigh and leg.

Visit http://www.nasalcleanse.com/index.html after watching our video on nasal irrigation as a natural sinus infection remedy. Learn how & why this natural sinus remedy really works! Unlike the messy, old-fashioned neti pot or competitors with badly-designed, backflow-prone squeeze bottles that can cause sinus infection, NasalCare’s patented NasalCare® Nasal Rinse System ensures comfortable and effective delivery throughout the nasal passages, preventing sinus infection, allergy and post nasal drip. A soothing mix of sea salt and Aloe Vera extract washes away nasal irritants and the common causes of colds and flu while providing nasal congestion relief via our nasal wash. NasalCare also acts as a sinus rinse for allergy treatment. Though used for centuries in the Orient as a natural remedy and preventative measure for all sinus conditions, nasal irrigation is just catching on here. Catch us now and stop catching colds and the flu! Learn more at: http://www.nasalcleanse.com/index.html.

Neurotransmitter 3D Animation
on Tuesday, December 21, 2010
Neurotransmitters are endogenous chemicals which transmit signals from a neuron to a target cell across a synapse. Neurotransmitters are packaged into synaptic vesicles clustered beneath the membrane on the presynaptic side of a synapse, and are released into the synaptic cleft, where they bind to receptors in the membrane on the postsynaptic side of the synapse. Release of neurotransmitters usually follows arrival of an action potential at the synapse, but may also follow graded electrical potentials. Low level "baseline" release also occurs without electrical stimulation. Neurotransmitters are synthesized from plentiful and simple precursors, such as amino acids, which are readily available from the diet and which require only a small number of biosynthetic steps to convert. The chemical identity of neurotransmitters is often difficult to determine experimentally. For example, it is easy using an electron microscope to recognize vesicles on the presynaptic side of a synapse, but it may not be easy to determine directly what chemical is packed into them. The difficulties led to many historical controversies over whether a given chemical was or was not clearly established as a transmitter. In an effort to give some structure to the arguments, neurochemists worked out a set of experimentally tractable rules. According to the prevailing beliefs of the 1960s, a chemical can be classified as a neurotransmitter if it meets the following conditions: * There are precursors and/or synthesis enzymes located in the presynaptic side of the synapse. * The chemical is present in the presynaptic element. * It is available in sufficient quantity in the presynaptic neuron to affect the postsynaptic neuron; * There are postsynaptic receptors and the chemical is able to bind to them. * A biochemical mechanism for inactivation is present. There are many different ways to classify neurotransmitters. Dividing them into amino acids, peptides, and monoamines is sufficient for some classification purposes. Major neurotransmitters: * Amino acids: glutamate, aspartate, D-serine, γ-aminobutyric acid (GABA), glycine * Monoamines and other biogenic amines: dopamine (DA), norepinephrine (noradrenaline; NE, NA), epinephrine (adrenaline), histamine, serotonin (SE, 5-HT), melatonin * Others: acetylcholine (ACh), adenosine, anandamide, nitric oxide, etc. In addition, over 50 neuroactive peptides have been found, and new ones are discovered regularly. Many of these are "co-released" along with a small-molecule transmitter, but in some cases a peptide is the primary transmitter at a synapse. β-endorphin is a relatively well known example of a peptide neurotransmitter; it engages in highly specific interactions with opioid receptors in the central nervous system. Single ions, such as synaptically released zinc, are also considered neurotransmitters by some[by whom?], as are some gaseous molecules such as nitric oxide (NO) and carbon monoxide (CO). These are not classical neurotransmitters by the strictest definition, however, because although they have all been shown experimentally to be released by presynaptic terminals in an activity-dependent way, they are not packaged into vesicles. By far the most prevalent transmitter is glutamate, which is excitatory at well over 90% of the synapses in the human brain. The next most prevalent is GABA, which is inhibitory at more than 90% of the synapses that do not use glutamate. Even though other transmitters are used in far fewer synapses, they may be very important functionally—the great majority of psychoactive drugs exert their effects by altering the actions of some neurotransmitter systems, often acting through transmitters other than glutamate or GABA. Addictive drugs such as cocaine and amphetamine exert their effects primarily on the dop

Operation ofInguinal hernia repair without mesh, Desarda Repair, no recurrence, pain, no mesh hernia surgery, hernia operation, no mesh, without mesh, hernia operation, hernia surgery, new method.

Appendicitis is caused by an infected appendix and requires appendectomy surgery. Here's more information on appendicitis and appendectomy.

More videos on my youtube channel

Carpal Tunnel Syndrome Information
Gene Causing Breast Cancer Resistance to Chemotherapy
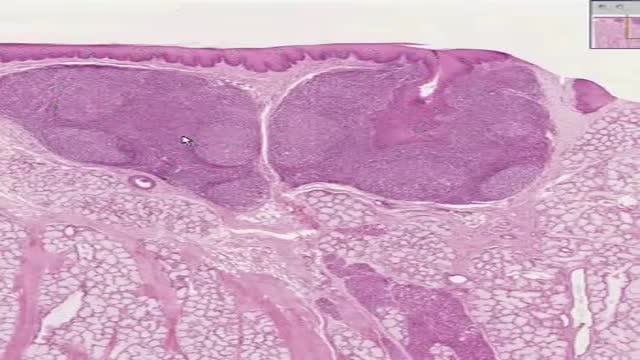
Histology of lingual Tonsil
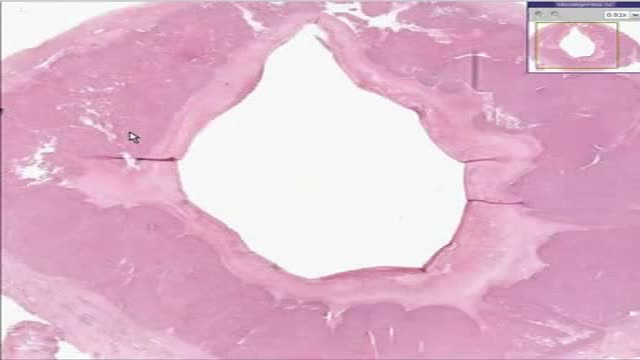
Histology of Corpus Luteum 2

Take Pregnancy Test Childbirth HD

Creating polidocanol foam

Eye Cyst Removal By Vitrectomy
