- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
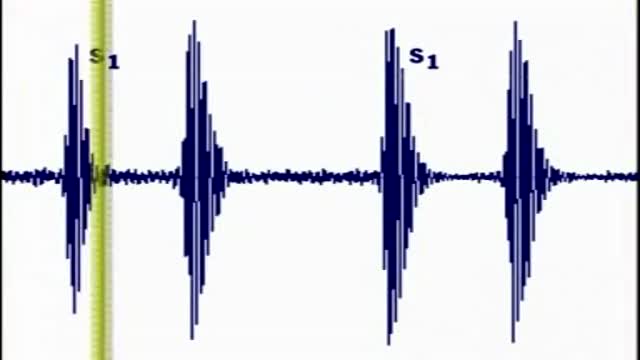
Heart sounds are the noises generated by the beating heart and the resultant flow of blood through it. Specifically, the sounds reflect the turbulence created when the heart valves snap shut. In cardiac auscultation, an examiner may use a stethoscope to listen for these unique and distinct sounds that provide important auditory data regarding the condition of the heart. In healthy adults, there are two normal heart sounds often described as a lub and a dub (or dup), that occur in sequence with each heartbeat. These are the first heart sound (S1) and second heart sound (S2), produced by the closing of the atrioventricular valves and semilunar valves, respectively. In addition to these normal sounds, a variety of other sounds may be present including heart murmurs, adventitious sounds, and gallop rhythms S3 and S4. Heart murmurs are generated by turbulent flow of blood, which may occur inside or outside the heart. Murmurs may be physiological (benign) or pathological (abnormal). Abnormal murmurs can be caused by stenosis restricting the opening of a heart valve, resulting in turbulence as blood flows through it. Abnormal murmurs may also occur with valvular insufficiency (regurgitation), which allows backflow of blood when the incompetent valve closes with only partial effectiveness. Different murmurs are audible in different parts of the cardiac cycle, depending on the cause of the murmur.
Obstructive lung disease is a category of respiratory disease characterized by airway obstruction. Many obstructive diseases of the lung result from narrowing of the smaller bronchi and larger bronchioles, often because of excessive contraction of the smooth muscle itself. It is generally characterized by inflamed and easily collapsible airways, obstruction to airflow, problems exhaling and frequent medical clinic visits and hospitalizations. Types of obstructive lung disease include; asthma, bronchiectasis, bronchitis and chronic obstructive pulmonary disease (COPD). Although COPD shares similar characteristics with all other obstructive lung diseases, such as the signs of coughing and wheezing, they are distinct conditions in terms of disease onset, frequency of symptoms and reversibility of airway obstruction.[1] Cystic fibrosis is also sometimes included in obstructive pulmonary disease
In an autologous transplant, a patient's own blood-forming stem cells are collected. He or she is then treated with high doses of chemotherapy, or a combination of chemotherapy and radiation. The high-dose treatment kills cancer cells, but also eliminates the blood-producing cells that are left in the bone marrow.

Physiological & pathological breath sounds
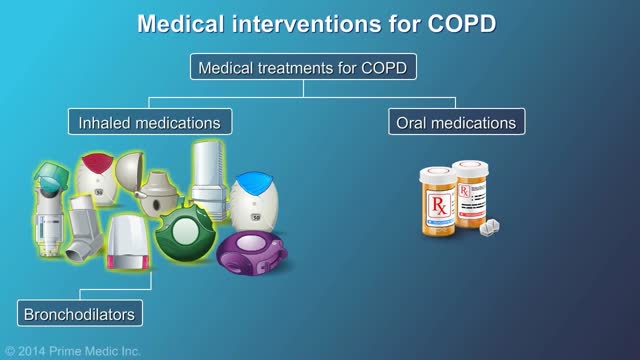
This Video COPD, or chronic obstructive pulmonary (PULL-mun-ary) disease, is a progressive disease that makes it hard to breathe. "Progressive" means the disease gets worse over time. COPD can cause coughing that produces large amounts of mucus (a slimy substance), wheezing, shortness of breath, chest tightness, and other symptoms. Cigarette smoking is the leading cause of COPD. Most people who have COPD smoke or used to smoke. Long-term exposure to other lung irritants—such as air pollution, chemical fumes, or dust—also may contribute to COPD.
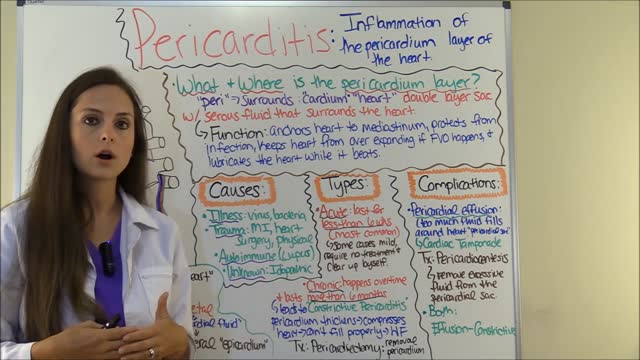
Pericarditis is an inflammation of the lining surrounding the heart (the pericardial sac). Pericardial effusion is a collection of fluid in the pericardial sac. This fluid may be produced by inflammation. The cause of pericarditis in most individuals is unknown but is likely due to viral infection.

Tampon for The First Time

More than 1 million Americans suffer a heart attack every year. Traditional symptoms—chest pain or pressure, cold sweat, extreme weakness—are well known. But there are more subtle signs you’re having or are about to have a heart attack that can be easy to miss. If you experience any of the following symptoms, see a doctor. Noticing heart attack signs early and getting prompt treatment can save your life.

A spider nevus is a collection of small, dilated arterioles (blood vessels) clustered very close to the surface of the skin. The cluster of vessels is web-like, with a central spot and radiating vessels.

The management of acute ischemic stroke has advanced greatly over the past 2 decades. New interventions, including intravenous and endovascular treatment strategies, have evolved to recanalize arteries and salvage the ischemic brain. The evolution of interventional approaches to the treatment of acute stroke has been prompted by the limitations of intravenous therapy and intended to extend the treatment window, improve recanalization rates, and subsequently long-term clinical outcomes. The major techniques that have defined the current field of interventional acute stroke management and the relevant past and current data, and ongoing clinical trials on interventional stroke therapy will be reviewed. New issues, such as futile recanalization, and time to microcatheter, will also be discussed.
The best way to prevent hepatitis A is through vaccination with the hepatitis A vaccine. Vaccination is recommended for all children age 12 months or older, for travelers to certain countries, and for people at high risk for infection with the virus. The hepatitis A vaccine is given as two shots, six months apart.
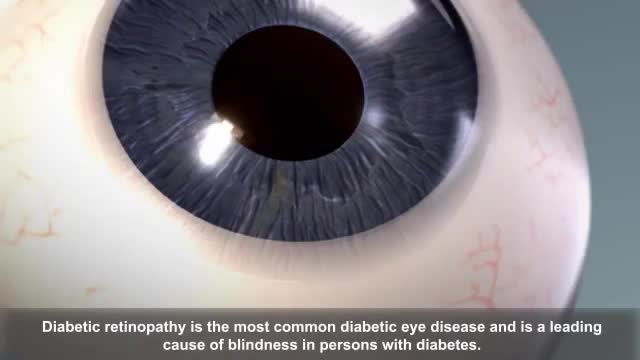
Diabetic retinopathy (die-uh-BET-ik ret-ih-NOP-uh-thee) is a diabetes complication that affects eyes. It's caused by damage to the blood vessels of the light-sensitive tissue at the back of the eye (retina). At first, diabetic retinopathy may cause no symptoms or only mild vision problems. Eventually, it can cause blindness. The condition can develop in anyone who has type 1 or type 2 diabetes. The longer you have diabetes and the less controlled your blood sugar is, the more likely you are to develop this eye complication.
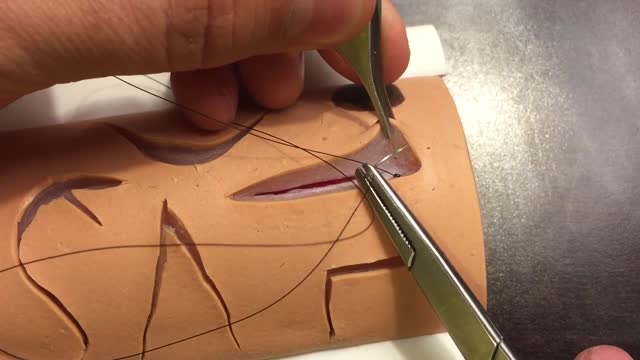
The two biggest considerations when choosing a suture are the location and tension of the wound. Other important considerations are tensile strength, knot strength, handling, and tissue reactivity. Sutures are divided into two major groups: Absorbable – lose the majority of their tensile strength in less than 60 days. They are generally used for buried sutures and do not require removal. Non-absorbable – maintain the majority of their tensile strength for more than 60 days. They are generally used for skin surface sutures and do require removal postoperatively. Suture needles also come in a variety of shapes and sizes. Curved needles are almost exclusively used in dermatological surgery. Cutting needles move through the tissue more easily and may have their primary cutting edge on the inside of the curve (conventional cutting) or outside of the curve (reverse cutting). The benefit of reverse cutting is that the tapered puncture left by the suture is directed away from the wound edge and therefore tissue tearing is less common. Non-cutting round needles cause even less tissue tearing and may be especially useful in delicate areas and fascia.

Traumatic brain injury (TBI) is a nondegenerative, noncongenital insult to the brain from an external mechanical force, possibly leading to permanent or temporary impairment of cognitive, physical, and psychosocial functions, with an associated diminished or altered state of consciousness.
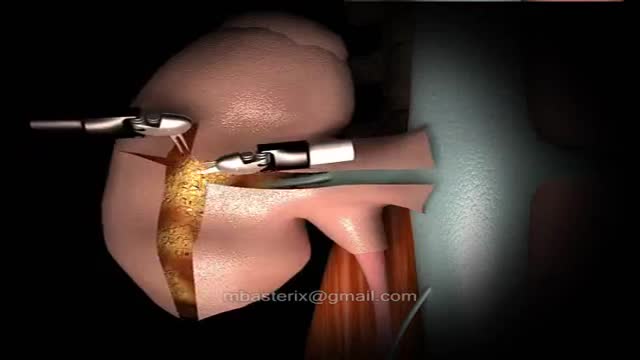
The robotic approach to renal surgery, particularly partial nephrectomy, has some inherent challenges, and some familiarity with the da Vinci robotic system is necessary. The surgeon must gain an understanding of the robotic arm movements and range of motion, especially in relation to the clutch and camera. The advent of robotically assisted prostatectomy in 2001 [23] paved the way for widespread accessibility to the da Vinci robotic unit and its application to renal surgery. Since that time, at least one multi-institutional survey has demonstrated superiority of the robotic approach when compared to laparoscopic for outcomes of blood loss, hospital stay and a substantially shorter warm ischemia time, while maintaining equivalence in positive margin rate, operative time and complications. [11] A transperitoneal approach is most commonly used. Prior abdominal operation is not necessarily a contraindication to this procedure, but access should be approached with regard for previous operation(s) by an experienced team.

Euthyroid sick syndrome (ESS), sick euthyroid syndrome (SES), thyroid allostasis in critical illness, tumours, uremia and starvation (TACITUS), non-thyroidal illness syndrome (NTIS) or low T3 low T4 syndrome is a state of adaptation or dysregulation of thyrotropic feedback control where the levels of T3 and/or T4 are ...

A blood transfusion is a routine medical procedure that can be lifesaving. During a blood transfusion, donated blood is added to your own blood. A blood transfusion may also be done to supplement various components of your blood with donated blood products. In some cases, a blood transfusion is done with blood that you've donated ahead of time before you undergo elective surgery. During a typical blood transfusion, certain parts of blood are delivered through an intravenous (IV) line that's placed in one of the veins in your arm. A blood transfusion usually takes one to four hours, though in an emergency it can be done much faster.

ADC was first identified early in the AIDS epidemic as a common and novel CNS syndrome.(4,5) The three components of the term, AIDS dementia complex embody central features of the condition. AIDS emphasizes its morbidity and poor prognosis, particularly when its severity is at stage 2 or greater (see Table 1), a severity comparable to other clinical AIDS-defining complications of HIV-1 infection. Dementia designates the acquired and persistent cognitive decline with preserved alertness that usually dominates the clinical presentation and determines its principal disability. Complex emphasizes that this disease not only impairs the intellect, but also concomitantly alters motor performance and, at times, behavior. This involvement of the nervous system beyond cognition is evidence of a wider involvement of the CNS than occurs in some other types of dementia such as Alzheimer's disease. Additionally, myelopathy may be an important, indeed predominating, aspect of ADC, and organic psychosis may also be a feature in a subset of patients (see Rheumatologic and Musculoskeletal Manifestations of HIV). These manifestations are therefore also encompassed within this term. By contrast, neither neuropathy nor functional psychiatric disturbance are included in ADC.

New Device can keep heart beating perfectly forever
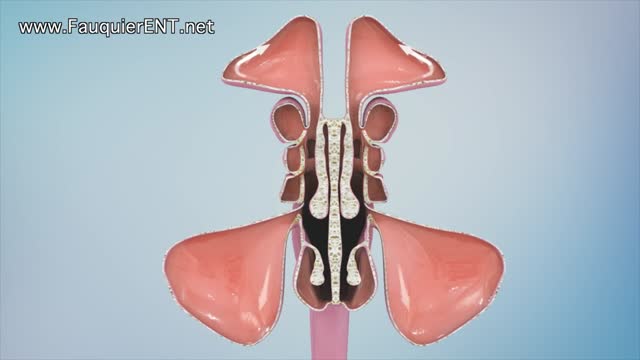
Sinusitis and Sinus Surgery Explained (Balloon Sinuplasty and Endoscopic Sinus Surgery)
