- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

some knowledge
An old video showing how to give an enema

Watch that Baby delivery Surgery video

The head-to-toe assessment in nursing is an important physical health assessment that you'll be performing as a nursing student and nurse.
Head-to-toe assessments allow nurses to assess the health status of patients by following a checklist of criteria.
On the job, your head-to-toe nursing assessment will be performed much faster, and it may be different or more specialized to accommodate the patients' needs within your nursing specialty.
This assessment represents a general assessment checklist (or cheat sheet) that you might encounter in nursing school. (Note: Always follow your instructor's requirements or your employer's assessment protocols).
This nursing head-to-toe examination video guide will focus on the following areas/skills:
-Vital Signs (pulse rate, respiration rate, temperature, oxygen saturation, blood pressure, pain assessment)
https://www.youtube.com/watch?v=gUWJ-6nL5-8
-Cranial Nerve examination
-Head assessment (hair, cranium, eyes, nose, mouth, ears, sinuses)
-Neck assessment (jugular vein, thyroid, trachea, carotid)
-Heart sounds assessment: https://www.youtube.com/watch?v=H48WsyIjFs0&t=73s
-Lung sounds assessment: https://www.youtube.com/watch?v=KNrcG077brQ
-Abdominal assessment
-Assessing extremities (arms, hands, legs, feet)
-Back assessment
-and more
While performing your comprehensive head-to-toe assessment, you'll want to record your findings in the documentation.
Nursing Gear: https://teespring.com/stores/registerednursern
Subscribe: http://www.youtube.com/subscri....ption_center?add_use
Notes: http://www.registerednursern.c....om/head-toe-assessme
Nursing School Supplies: http://www.registerednursern.c....om/the-ultimate-list
Visit our website RegisteredNurseRN.com for free quizzes, nursing care plans, salary information, job search, and much more: http://www.registerednursern.com
Check out other Videos: https://www.youtube.com/user/R....egisteredNurseRN/vid
All of our videos in a playlist: https://www.youtube.com/watch?v=pAhHxt663pU&list=PLQrdx7rRsKfXMveRcN4df0bad3ugEaQnk
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Study Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Tips & Questions" https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Types of Nursing Specialties: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Healthcare Salary Information: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
New Nurse Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Career Help: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
EKG Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Dosage & Calculations for Nurses: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Diabetes Health Managment: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf

-The cremasteric reflex test is considered positive if there is elevation of the testis in response to stroking the upper inner thigh. This reaction is typically absent in testicular torsion and boys under the age of 6 months. Although not completely reliable in older boys and adults, an absent cremasteric reflex is highly suggestive of torsion. Patients with epididymitis usually have a normal cremasteric reflex, with pain and swelling isolated to

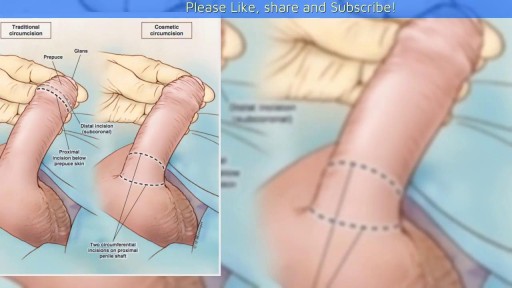
A video showing the circumcision of a male baby

CORRECTION: After review of this video, it is clear that this video is of a baby who is near full term (40 weeks) based on the size. Late trimester "abortions" are defined only to viability of a baby (24 weeks) A 24 week baby is much smaller than this baby shown and by definition this is not a late "abortion" procedure. The proper labeling of this video should be management of a deceased breech baby with "head entrapment" as this was almost certainly a naturally occuring delivery and an OB nightmare (Reviewed by Dr. Frederick Bright)

Morning erections have colloquially been termed as “morning wood” while scientifically it is called nocturnal penile tumescence. It is a normal and healthy physiological reaction and response that most men experience in their lives. Morning erections are really the ending of a series of erections that happen to men during the night. Healthy men can, on average, have anywhere between three to five erections in a full night of sleep, each of which lasts from 25-35 minutes.

Armpit Abscess Drainage
Recto-vaginal medical examination
During the examination, the doctor gently puts a lubricated, gloved finger of one hand into the rectum. He or she may use the other hand to press on the lower belly or pelvic area. A digital rectal exam is done for men as part of a complete physical examination to check the prostate gland .

watch that video of Popping a Huge Hand Burn Blister

"The act of cutting off the prepuce or foreskin of males, or the internal labia of females." Webster's Revised Unabridged Dictionary (1913)

Vaginal Speculum and Bimanual Exam
Ever wonder How Male to Female Trans'Gender Surgery works?

Circumcision by Dissection method

Watch that video of Popping Huge Epidermoid Cyst

The big bang is the moment when the uterus, vagina, and anus contract simultaneously at 0.8-second intervals. A small orgasm may consist of three to five contractions; a biggie, 10 to 15. Many women report feeling different kinds of orgasms
