- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
![Female Foley Insertion (Urinary Catheter) [How to Insert Nursing Skills]](https://i.ytimg.com/vi/Mq4Yh0-iozY/maxresdefault.jpg)
Pass your tests and improve your grades with the below FREE resources:
1) A FREE 140 Must Know Meds book
Click here to get your FREE copy of the 140 Must Know Meds Book: https://bit.ly/41rxSt0
2) A FREE test-taking tips webinar
Join us for our free test-taking tips webinar to boost your exam scores: https://bit.ly/nursingtesttaking
You can now test your knowledge with a free lesson quiz on NURSING.com!
Click here to take a free quiz: https://bit.ly/3HwJr8t
FREE Nursing School Cheat Sheets at: http://www.NURSING.com
Get the full lesson on Female Foley Insertion here:
https://nursing.com/lesson/ski....lls-03-01-inserting-
Get the Male Foley Insertion lesson here:
https://nursing.com/lesson/ski....lls-03-02-inserting-
Get the Sterile glove application lesson here:
https://nursing.com/lesson/ski....lls-01-04-sterile-gl
Check out our new Nurse Care Plan Lessons here:
https://bit.ly/3BPRfPL
Get Access to Thousands of Lessons here:
https://nursing.com/courses/
Welcome to the NURSING Family, we call it the most supportive nursing cohort on the planet.
At NURSING.com, we want to help you remove the stress and overwhelm of nursing school so that you can focus on becoming an amazing nurse.
Check out our freebies and learn more at: (http://www.nursing.com)
Female Foley Insertion (Urinary Catheter)- Nursing Skills
In this video, we’re going to look at inserting a Foley catheter in a female. Of course make sure you’ve verified your order and told the patient what’s happening. You’ll also typically want to perform perineal care before you start. Then, you’ll want to assist the patient into the appropriate position. For females, that’s supine with their knees bent and feet close to their hips – allowing their knees to fall to the side. You may need a helper to help hold the patient in this position. We love you guys! Go out and be your best selves today! And, as always, happy nursing!
Bookmarks:
0.05 Female Foley insertion introduction
0.15 Patient positioning
0.27 Opening the sterile kit
1.41 Setting up the sterile field
2.25 Prepping the remaining Foley kit items
2.34 Catheter lubrication
3.00 Saline syringe attachment
3.10 Iodine, swabs and cleansing the area
3.52 Catheter insertion (into urethra)
4.06 Balloon inflation
4.25 Final catheter setting
4.31 Securing the catheter and bag
4.48 Discarding your supplies
5.00 Documentation
5.08 Foley insertion outro
Visit us at https://nursing.com/medical-disclaimer/ for disclaimer information.
NCLEX®, NCLEX-RN® are registered trademarks of the National Council of State Boards of Nursing, INC. and hold no affiliation with NURSING.com.

Another video showing different technique of child birth

Proctoscopy in Jackknife Position for examination of the rectum

Calcified Brain Abcess complete removal,
surgery

Medical breast examination of a female from Loyola University,Chicago

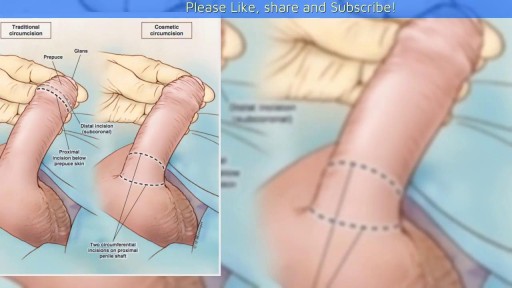
Adult circumcision video

http://plantar-fasciitis-solution.info-pro.co Foot Arch Pain, Sharp Pain In Heel, Pain In Foot, Achilles Heel Pain, Chronic Plantar Fasciitis What is Plantar Fasciitis? Plantar fasciitis is a common injury that affects the heel of a person’s foot. The arches of the feet are supported by a tough and fibrous tissue known as the plantar fascia and when this tissue is used repetitively, injury may occur. It can be easy to overuse the feet, especially when participating in activities such as sporting events. Hence, plantar fasciitis is more commonly found in athletes or others who are constantly using their feet for long durations. With excessive use, the planar fascia will eventually give in and this condition may also be progressive. Runners and those who are known to participate in similar activities need to ensure that they do not damage this important band of tissue. In addition, body weight could be a factor that leads to the occurrence of plantar fasciitis. If a person is overweight, the feet and subsequently the plantar fascia tissue could become overwhelmed. Improper footwear could also cause a strain on the plantar fascia tissue and this could gradually become severe over time. plantar fasciitis relief in 7 days click here. http://plantar-fasciitis-solution.info-pro.co

Dr. Arthur Handal explains both an open and closed approach to a Rhinoplasty and which is more effective, in his opinion.

Knee pain location can often tell you what type of knee pain you have. If you confirm that with common symptoms and what aggravates it… you can get a pretty good idea of ‘why my knee hurts’. So, here’s a quick look at the most common type of knee problems.
‘The 3 Essential Exercises EVERYONE Should Do’ … Watch this EXCLUSIVE video, only here: https://stefan-becker.mykajabi.com/3-essentials
QUESTIONS? I answer questions here now: I’ve started a Facebook Group to help people achieve their musculo-skeletal goals. Join here… https://www.facebook.com/groups/bodyfixexercises
AND I’m developing a Coaching Program! Over 12 weeks, I help people with posture related issues—like neck, shoulder, & upper back pain—discover their root problem and correct it using science-backed mobilising, stretching, & strengthening exercises… so they can feel straight, strong, flexible, & pain free again (and get back to doing what they love). Find out more, and join the wait list here… https://stefan-becker.mykajabi.com/waiting-list
0:00 Intro
0:11 Pain at the front of the knee (Pain in kneecap)
0:42 Pain below kneecap
1:40 Pain on inside of knee
3:05 Pain below knee on inside
3:29 Pain on outside of knee
3:28 Pain above knee
3:28 Pain behind knee
---------------------------------------
Mentioned in this video...
How To Fix Pain In The Front Of The Knee… (Runner's Knee) https://youtu.be/g0qmx_0enAA
Looking to stop your knee problems? Do this...
Knee Strengthening Exercises To Prevent Knee Pain
https://youtu.be/Pk-ae_lyx7M
How To Treat Patellar Tendinopathy (Jumper’s Knee) & Quadriceps Tendinopathy
https://youtu.be/MkPwsb-rQwU
---------------------------------------
If you’re asking yourself ‘what’s the cause of my knee pain?’ or ‘what kind of knee pain do I have?’ (so that you can look up solutions to your knee pain on YouTube) the position of your knee pain will tell you a lot.
THE MOST COMMON KNEE PAIN TYPES?
Knee pain during running (or actually kneecap pain while running) is usually just that… Runner’s Knee (PATELLOFEMORAL PAIN SYNDROME, or it’s old name: Chondromalacia Patella) If you get knee pain while cycling it will often be the same thing. Same with knee pain with stairs.
Knee pain while squatting could be Runner’s Knee, but if you get pain in the tendon below the kneecap, it’s more likely to be Patellar Tendonitis or Jumper’s Knee.
Meniscus Tears will give you pain on the inside of the knee that is a localised pain, can feel as if it gets stuck, or feel like it’s going to give way, and often it’s hard to fully straighten or fully bend your knee.
Knee pain on the outside of the knee is usually Iliotibial Band Syndrome
ALSO COVERED:
Infrapatellar Fat Pad Syndrome (Hoffa's Syndrome)
Osgood-Schlatter Disease
Medial Collateral Ligament Tear
Iliotibial Band Syndrome
Osteoarthritic Knee Pain
Pes Anserine Bursitis.
Quadriceps Tendinopathy
Popliteus Strain
Baker’s Cyst
ACL Or PCL Tear/Rupture
------------------------------------
#bodyfixexercises #kneepainrelief #kneepain

Surgeons at The Children’s Hospital of Philadelphia were the first to perform a bilateral hand transplant on a child. Our research and work in this groundbreaking field of medicine led us to establish the Hand Transplantation Program. Combining the expertise of the Penn Transplant Institute and the Hospital’s Division of Plastic and Reconstructive Surgery and Division of Orthopedics, the program aims to improve quality of life for children who may benefit from this procedure. This is Zion, one year after the surgery
The condition is caused by a blockage in the lymphatic system, part of the immune and circulatory systems. Lymphedema is most commonly caused by lymph node removal or damage due to cancer treatment. The main symptom is swelling in an arm or leg that may be accompanied by pain or discomfort. Exercise, wrapping, massage, and compression can help.

Watch that Female to Male Gender Changing Surgery


some knowledge

Proctoscope rectal examination

Watch that video of Mystery of Ice Frozen woman came back to life

This poor old lady came with swelling in her left buttock for 10 days.She had history of injection in her buttocks two weeks back. She developed painful swelling and redness in her left gluteal region with difficulty in walking.It was diagnosed as injection abscess left gluteal region which needs incision and drainage under local anesthesia.Patient part painted and drapped.2% Lignocaine with adrenaline was infiltrated around the swelling for proper filed block.I use no-11 blade for stab incision over the swelling at the most fluctuating point of the abscess.You can watch how pus was flowing out from the cavity.The aim is to drain all pus from the abscess cavity.Finger exploration is essential to break all loculi inside the cavity, to know the depth and extend of the cavity and to fascilitate proper drainage of residual pus.after pus evacuation,, the cavity should be irrigated with normal saline and betadine solution.lastly the cavity to be packed with betadine soaked guage pieces.Proper dressing is essential.the dressing to be changed after 24 hours.daily dressing is essential with a good antibiotic coverage.the cavity usually obliterates within a period of seven to ten days.

How to Collect Blood Cultures
Video of the technique and early outcomes of Robotic Assisted Microsurgical Vasectomy Reversal at University of Florida and Shands, Gainesville, Fl, by Dr. Sijo Parekattil.
