- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Benny Hill Crazy hospital
They were victims of caisson disease. This condition, also known as the bends or decompression sickness, is caused by the formation of gas bubbles in the body. Human body tissues contain small amounts of the gases present in the air.
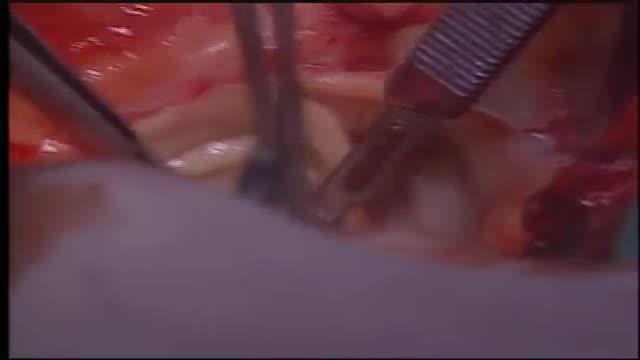
Surgery to replace an aortic valve is done for aortic valve stenosis and aortic valve regurgitation. During this surgery, the damaged valve is removed and replaced with an artificial valve. The valve replacement is typically an open-heart surgery.
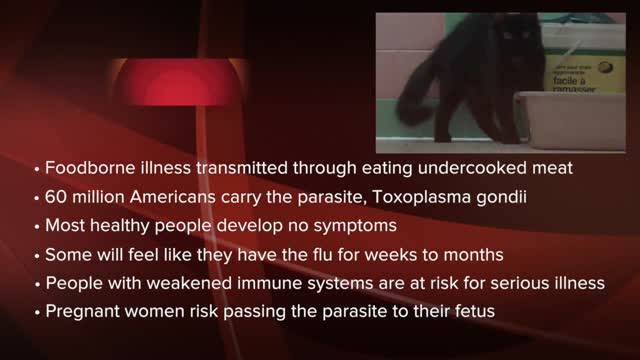
Toxoplasmosis (tok-so-plaz-MOE-sis) is a disease that results from infection with the Toxoplasma gondii parasite, one of the world's most common parasites. Toxoplasmosis may cause flu-like symptoms in some people, but most people affected never develop signs and symptoms. For infants born to infected mothers and for people with weakened immune systems, toxoplasmosis can cause extremely serious complications. If you're generally healthy, you probably won't need any treatment for toxoplasmosis. If you are pregnant or have lowered immunity, certain medications can help reduce the infection's severity. The best approach, though, is prevention.
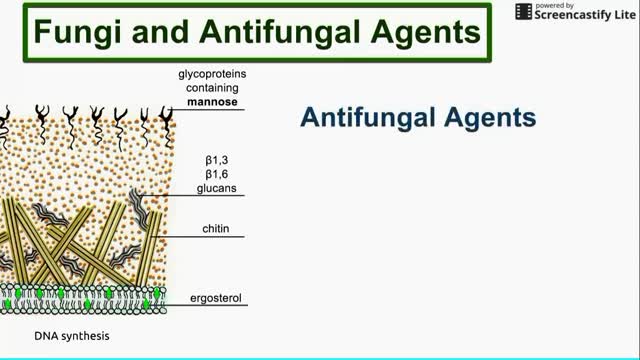
This is a brief overview of antifungal agents, their mechanisms of action, and some fungi that they affect.

The most detailed explanation you'll ever hear on what makes some people's feet stink. (Not yours, obviously.)

Given the common presentation of onychodystrophy, physicians should have a firm grasp of common presentations of conditions like onychomycosis, trachyonychia and psoriasis. Accordingly, this author reviews keys to effective diagnosis and pertinent treatment considerations. Nail cosmesis and discomfort are the main motivators for most of our patients to schedule a podiatric consultation. During that patient visit, it is important for the podiatric practitioner to delve into the cause of the problematic nail change, known as onychodystrophy. Onychodystrophy, which is any alteration of nail morphology, encompasses a wide spectrum of nail disorders. Caused by either exogenous or endogenous factors, nail dystrophy may manifest as a misshapen, damaged, infected or discolored nail unit that may affect the toenails, fingernails or both.
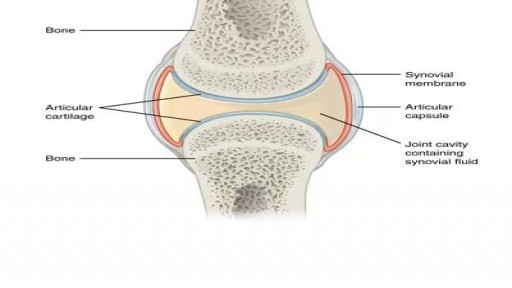
What happens when you crack your joints?

http://plantar-fasciitis-solution.info-pro.co Foot Arch Pain, Sharp Pain In Heel, Pain In Foot, Achilles Heel Pain, Chronic Plantar Fasciitis What is Plantar Fasciitis? Plantar fasciitis is a common injury that affects the heel of a person’s foot. The arches of the feet are supported by a tough and fibrous tissue known as the plantar fascia and when this tissue is used repetitively, injury may occur. It can be easy to overuse the feet, especially when participating in activities such as sporting events. Hence, plantar fasciitis is more commonly found in athletes or others who are constantly using their feet for long durations. With excessive use, the planar fascia will eventually give in and this condition may also be progressive. Runners and those who are known to participate in similar activities need to ensure that they do not damage this important band of tissue. In addition, body weight could be a factor that leads to the occurrence of plantar fasciitis. If a person is overweight, the feet and subsequently the plantar fascia tissue could become overwhelmed. Improper footwear could also cause a strain on the plantar fascia tissue and this could gradually become severe over time. plantar fasciitis relief in 7 days click here. http://plantar-fasciitis-solution.info-pro.co

Watch that video of a Man Impaled by Shovel In His Butt Inside ER

Watch that video of Gross Teeth Full of Worms Removal
Come Si Può Rimanere Incinta, Rimanere Incinta A 42 Anni Naturalmente, Settimane Di Gravidanza--- http://come-rimanere-incinta.info-pro.co --- Come rimanere incinta in modo naturale La sterilità può essere generalmente definita come l'incapacità di avere una gravidanza dopo aver provato per almeno un anno senza l'uso di contraccettivi. Nei paesi occidentali la sterilità colpisce circa il 15% della popolazione. Mentre c'è chi cerca di concepire con metodi alternativi come la fecondazione in vitro, altri preferiscono ottimizzare le probabilità di rimanere incinta naturalmente. Cercare di rimanere incinta naturalmente può essere molto importante dal momento che molte coppie o individui con diagnosi di sterilità possono tornare ad essere fertili senza trattamenti (e quindi si dovrebbe parlare di "sub-fertilità" piuttosto che di "sterilità"). Quando si cerca di rimanere incinta naturalmente, il fattore più importante è capire il ciclo mestruale e la tempistica di ovulazione, che porta ad ottimizzare le possibilità di ottenere una gravidanza. Di solito l'ovulazione avviene intorno al quattordicesimo giorno e, di conseguenza, per ottenere una gravidanza naturale la coppia dovrebbe avere più rapporti sessuali possibili tra il dodicesimo e il quindicesimo giorno. Ogni donna ha un ciclo leggermente diverso. Per cui, per migliorare le probabilità di rimanere incinta, è indispensabile studiare i propri cicli e calcolare con esattezza quando si ovula. L'antico Sistema Olistico Cinese In 5-passi Per Rimanere Incita Naturalmente E Avere Bimbi Sani Clicca sul link http://come-rimanere-incinta.info-pro.co

Hair Regrowth, Home Remedies For Hair Fall And Regrowth, Hair Regrowth Supplements---- http://hairlossblackbook.plus101.com/ --- Best Hair Loss Treatment for Men , Looking for the best hair loss treatment for men? Then don’t be surprised to find that there are actually not that many. The reason is very simple – each individual will have his own idea on what is considered to be the best treatment due to varying reasons and factors. For some, it might be the use of conventionally developed creams; others find medicated shampoos to be the solution, while others still think that there is no better treatment aside from hair transplant. Sure, hair transplants are indeed effective, but not many can afford the cost and conventional medications might bring about various side effects as well. Men generally play a hit or miss game where hair loss is concerned, heading for the next biggest fad in hair loss prevention and hoping that they themselves will get the solution that they have been hoping for. But what most men tend to miss is the fact that sometimes the best solution for their problem is already within their reach, they only fail to realize it due to the growing concern that they have regarding their problem. One of the most underestimated methods in treating hair would be the natural route. Many men do not even start considering using natural products until they have exhausted what is available in terms of conventional treatments and medications. Hair supplements like Ginseng, Horsetail, Nettle, Valerian, Zinc, Saw Palmetto, Black Currant Oil, Capsicum, Red Sage and others can be effectively used along with natural shampoos, creams, and gels to create an effective and highly individualized treatment that any individual will be able to benefit from. If you however would like to know more about the options available, one site that will be able to give you more facts and useful information would be, http://hairlossblackbook.plus101.com/ , so do check it out and start working on your best hair treatment approach today!

Watch that video of The Most Unbelievable Medical Condition

Watch that video of Removing Front Teeth

Watch that video of Doctors Removed 30 Pounds Of Poop From Man’s Colon
Home Remedies For Hair Fall And Regrowth, Hair Regrowth, Hair Regrowth Supplements--- http://how-to-regrow-your-hair.info-pro.co/ --- Male Hair Loss Solution, Millions of people all over the world are affected by hair loss, and it’s not only the males that suffer this condition as even females are affected by this problem. What’s sad is that many of the individuals affected by such a condition end up just accepting what is happening to their hair due to lack of information or options. Living their life hiding under cover from wigs or toupee’s when there are actually better options around the corner waiting for them. For males though losing their hair can be devastating, which is why many are sent scrambling for the next most effective male hair loss solution that they can get their hands on. There are actually many solutions that you can try if you want to stop your hair from falling out. Now, it’s a very big possibility that some of the methods that will be mentioned here you might have already heard of or even tried before, but, there is also a chance that you might be able to get an idea for an entirely new technique which will be able to help you out as well. So without further ado, here are some of the male hair loss solutions that you can try out: Block DHT: DHT is a hormone that is manufactured in the bloodstream due to excesses in the testosterone levels and is the main leading cause of male baldness. Simply put, DHT is a hormone that clings to your hair follicles and kills them – slowly. The three mentioned above are just for starters as well because there are so many more methods that you will be able to choose from when it comes to male hair loss solution. If you are looking for a definitive guide however, one can be found at http://how-to-regrow-your-hair.info-pro.co/
Bloating And Gas, Flatulence Remedy Ginger, Get Rid Of Gas And Bloating, Involuntary Flatulence--- http://flatulence-cure.plus101.com --- 7 tips on Flatulence Treatment and help you get rid of flatulence forever. 1. Flatulence is such a broad term, with so many connected and side issues, that it is rather short sighted to refer to it simply as "farting" - which so many people do. Certainly, the breaking of wind is the key identifier for flatulence. However, to merely concentrate on the noise and the smell of flatulence is to miss out on the important facts that govern its causes, its symptoms and its remedies. Picking the right flatulence treatment means needing to concentrate on the type of flatulence you have, the health issues surrounding it and the general health situation of the sufferer. 2. Be Realistic in Your Flatulence Treatment If the definition of flatulence was simply that you had wind a few times a day and occasionally broke wind in embarrassing situations, then flatulence treatment really would not be that much of a priority. However, the truth of the matter is that excessive flatulence will affect more than just social situations. It is thankfully uncommon enough to suffer from painful stomach flatulence, but that is not to say that it is something you should ever ignore. Your digestive system is vitally important for your health, and if problems arise then they need to be addressed with the right flatulence treatment. 3. When you are suffering from flatulence problems, you need to identify why it is a problem and what the problem can be traced back to. We all have flatulence every so often, most of us having wind at least once a day and usually more often. Getting rid of the gases that our system generates when digesting food is essential, as is finding a kind flatulence treatment - otherwise we would soon become quite unwell. It is how often you release those gases and how they are released that matters more than anything. The last thing you want is to have occasional, sporadic flatulence that hurts, smells foul or is particularly audible. 4. Gas is a by-product of digestion, and if you are not breaking wind at all then there is probably a problem. Excessive flatulence means that you are producing too much gas when digesting food, and means that your digestive system is not functioning as it should be. 5. Painful flatulence occurs when you are digesting the food badly, because the stomach is failing to break it down as smoothly as it should. It is not that uncommon to feel, perhaps, a little bit of burning flatulence - this can happen after too much spicy food - but if it is becoming the norm then it is something that needs to be addressed with the right flatulence treatments. 6. Keep A Note For Best Flatulence Treatment Results 7. By identifying which foods are connected with which problems, you can begin the right flatulence treatment. It is better to do this, and deal with the problem before it grows rather than trying to cure a bigger problem. Would you like to cure your gas problems and bloating today! Then you need to see this website below: http://flatulence-cure.plus101.com
Perdre Du Poids, Perte De Poids Rapide, Perdre Son Ventre, Pilule Pour Maigrir, Soupe Minceur ---- http://perte-poids-rapide.info-pro.co -- Comment maigrir sans efforts ? Maigrir sans efforts est la promesse de la plupart des régimes. Seulement, ce n’est pas souvent vraiment le cas. C’est tout simplement une promesse qui attire car nous sommes nombreux et nombreuses à rechercher la solution pour perdre du poids sans se prendre la tête ! Alors comment maigrir sans efforts ? Maigrir sans efforts c’est quoi au juste ? Tous ceux ou celles qui veulent se débarrasser de leurs kilos espèrent trouver comment y arriver sans avoir à faire des tonnes d’efforts. Maigrir est souvent compliqué et difficile. Il faut tenir et donc être motivé. La plupart des régimes demandent beaucoup d’efforts…trop d’efforts. Et c’est pourquoi la plupart ne marchent pas ou ne durent qu’un temps. Ils sont trop durs à tenir sur du long terme et soit on craque avant la fin de la méthode soit on reprend ses kilos aussi vite qu’ils sont partis. Alors pourquoi ne marchent-ils pas et pourquoi maigrir sans efforts est une réelle demande ? Parce que pour perdre du poids, ces régimes en demandent trop. Perdre du poids sans efforts c’est avant tout : Ne pas compter les calories de tout ce que l’on consomme Ne pas être frustré Ne pas se priver de tout ou de plusieurs groupes d’aliments Ne pas passer des heures à déchiffrer les étiquettes dans les magasins Ne pas se fixer des objectifs inatteignables Ne pas s’en vouloir dès que l’on fait un écart Ne pas s’isoler pour ne pas être tenté Lorsque l’on regarde cette liste, cela peut paraître impossible de maigrir sans faire d’efforts. Pourtant c’est tout à fait possible…. commencer à mincir sainement ET durablement maintenant ! Cliquez ici: http://perte-poids-rapide.info-pro.co

Anterior cruciate ligament reconstruction is a surgical tissue graft replacement of the anterior cruciate ligament, located in the knee, to restore its function after an injury.
