- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

You have a good hearing again baby
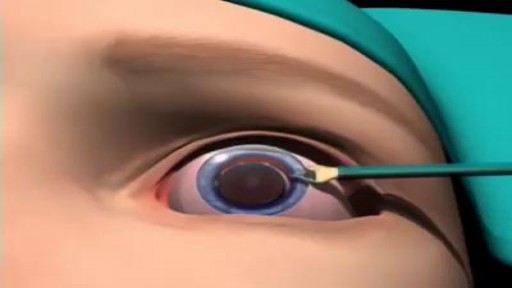
Most cataracts are associated with the aging process and are common among older Americans. In fact, according to the National Eye Institute (NEI), 68.3 percent of Americans 80 and older had cataracts in 2010. And the prevalence of cataracts in the U.S. is expected to grow significantly in the years ahead, due in part to the aging of the population. In 2010, roughly 24.4 million Americans had cataracts, and that number is projected to grow to 50.2 million by the year 2050, according to NEI.

A pacemaker insertion is the implantation of a small electronic device that is usually placed in the chest (just below the collarbone) to help regulate slow electrical problems with the heart.
Watch that video to know How To Increase Testosterone Levels Naturally
Appareil Pour La Cellulite, Creme Anti Cellulite Efficace, Anti Cellulite Maison, Café Cellulite--- http://perdre-sa-cellulite.plus101.com --- Cellulite Des Cuisses, Que Faire? Comment Eliminer Vite Sa Cellulite Des Cuisses Avec Des Exercices et L'alimentation cellulite-cuissesMême si la plupart des gens se mettent continuellement à la chasse de la cellulite, jusqu’à ce jour, il n’y a pas encore eu de remèdes miracles. Elle est particulièrement causée par le manque d’activités physiques et une alimentation non équilibrée. Elle apparaît souvent sur les fesses, les hanches et principalement sur les cuisses. Ainsi, pour se débarrasser de la cellulite surtout celle des cuisses, il est important d’avoir une alimentation équilibrée et de pratiquer des exercices sportifs. Il vous suffit de suivre les recommandations dans la vidéo ci-dessous qui vous aideront à tonifier vos jambes de manière efficaces, ainsi réduisant la présence de la cellulite sur les fesses, hanches et cuisses pour une silhouette plus attirante.CLIQUEZ ICI: http://perdre-sa-cellulite.plus101.com

Watch that video to know How To Increase Your Testosterone Levels Naturally

Women Heart Attack Symptoms, Healthy Living Tips, Heart Attack Symptoms Arm, Nutritional Tips, Heart.---- http://grow-younger-blood-good-info-co --- Why doctors let your family die One thing that keeps getting missed in that debate is how doctors, are so controlled by insurance companies, that they hold back from running life-saving blood tests. If you ever get a chance to ask a doctor, how he feels about HMO's, you'll get a glimpse into the sinister reality, of how corrupt and flat-out homicidal our healthcare system really is. This is why it's so important, to watch the new John video to get the REAL scoop on your health. It turns out that there are some life saving (or at least life-lengthening), tests you NEED to take but that doctors are not allowed to tell you about. And if you are under a big corporate health plan, you're even more likely to have been. cruelly lied to by the health industry. Watch this video. It's time to take your life and your family's health into your own hands. Once you have this information, no one not even the President himself can stop you Click Here. http://grow-younger-blood-good-info-co

one of the best videos I've ever seen..

Fast Lower Back Pain & Sciatica Pain Relief – Beginners Yoga Stretches and Poses


Eye Sclera Tattoo Procedure
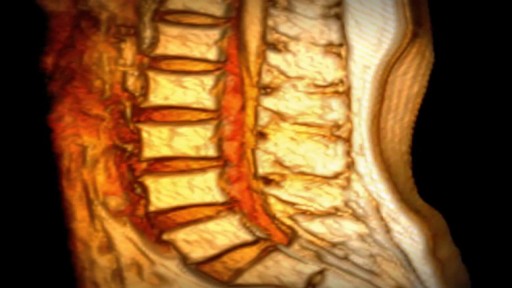
If you have been diagnosed with a bulging disc, you are not alone. Bulging discs, also known as a disc protrusion, are a very common occurrence. They usually remain asymptomatic; however, they can cause discomfort and disability in various parts of the body if the disc compresses an adjacent nerve root or the spinal cord. As we age, the outer fibrous portion of our discs can weaken. Pressure from the central core of the disc can then stretch to the outer rim, causing the disc to bulge. If left untreated, the disc can continue to bulge until it tears, which is classified as a herniated disc. Because a bulging disc does not always show symptoms, many people have bulging discs without realizing it. As long as the bulging area does not press against a nearby nerve, no symptoms occur. When the bulging disc does cause a pinched nerve, however, you may begin to experience symptoms. In the lower back, the damaged disc can cause pain to travel to the hips, buttocks, legs and feet. In the cervical spine, pain can radiate from the neck, down the arm and to the fingers.
Systemic lupus erythematous is an autoimmune condition characterised by damage to organ systems due to autoantibodies and immune complex deposition. Genes, epigenetic changes and environment play a role in its pathogenesis. SLE is a truly multi system disease causing widespread clinical manifestations in almost all organ systems. Autoantibodies in SLE are numerous and mainly include ANA, dsDNA, Sm and others.


Examination of the lymph nodes of the head

Positive Pressure Ventilation with a face mask and a bag-valve device

Video-Assisted thoracoscopy
Starting an IV
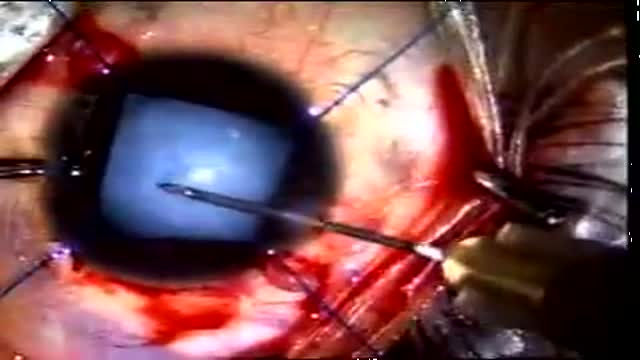
This video shows management of rupture of the posterior capsule post blunt trauma in a child aged 8. Pre-operative suspicion of PCR was strong because of a flat anterior. So we were careful in our approach from the very beginning. CCC was performed and then dry aspiration of lens matter initiated. Sice vitreous showed, so anterior vitrectomy was done along with systematic removal of the lens matter. An acrysof multi-component lens was implanted into the sulcus and optic captured into the CCC.Outcome was very good.
