- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Synthol, otherwise known as site enhancement oil is used by some people (including bodybuilders) to increase the apparent size of their muscles by directly injecting the oil into their muscle tissue. Users treat it as a short cut of looking like a body builder, without the actual hard work of bodybuilding training. With repeated injections, a larger volume of synthol builds up inside the muscle, expanding its size like a balloon filling up with air. Side effects of synthol can cause nerve damage, stroke, ulcers, pulmonary embolisms, and much more. Injecting synthol is very dangerous and if that doesn’t deter potential users, there is also a problem from an aesthetic standpoint; synthol use makes ones body look deformed (just see for yourself in the pictures below).

Computed tomography (CT)-guided transthoracic needle biopsy is a well-established, minimally invasive diagnostic tool for pulmonary lesions. Few large studies have been conducted on the diagnostic performance and adequacy for molecular testing of transthoracic core needle biopsy (TCNB) for small pulmonary lesions.

When placement of a urethral catheter is contraindicated or unsuccessful, percutaneous suprapubic urinary bladder catheterization is a commonly performed procedure to relieve urinary retention. [1, 2] This topic describes the Catheter over needle technique. The Seldinger technique is described in the Clinical Procedures topic Suprapubic Aspiration.
How to Improve Sexual Health or Stamina Part 4 All Solution of Male Disorder Male Infertility Diagnostic and Treatment Re-Slim Care Latest Technology in Pakistan Dr. Aslam Naveed is a well known sexologist in Pakistan. He has treated more than 1 Lac patients since last 30 years of clinical Practice in sexology, he knows how to help the people facing sexual disorders. Contact: 02134965050, 03432821919 https://www.facebook.com/menssexcareclinic/ ADDRESS: Men’s Care Modern Hospital, Opposite, Safari Park, University Road, Karachi, Pakistan.

Watch that video of The Worst skin Jiggers Removals

Podalic version is an obstetric procedure wherein the fetus is turned within the womb such that one or both feet present through the cervix during childbirth. It is used most often in cases where the fetus lies transversely or in another abnormal position in the womb.

Watch that video of Bodybuilder's Colon Contains 10 lbs of Meat Worms
Pain in joints or any part of body is very unpleasant and annoying experience. It is very common in people those suffering from arthritis. To get an end to all such pains, one can start using Generic Celebrex ( https://www.medexpressrx.com/celebrex-generic.aspx ). Here is a brief detail about this wonderful painkiller.

How to remove the Intra Uterine Device (IUD)

Labia minoraplasty is an elective procedure that can reduce the size and reshape the inner vaginal lips. Large or asymmetrical labia minora can leave you feeling self-conscience in tight clothing or during intimacy. Long labia may result in rubbing, irritation or discomfort during intercourse and exercise. Certain skin conditions can cause increased sensitivity or tearing of the labia minora. In some cases, the labia minora may be fused with tissue in the labia majora and require medical correction.

I talk about 5 Essential Skills you need as a nurse. These skills are timeless in the fat that you will always need to use them at some level. Of course specific skills are good to have as well but these skills are universal and can help you in other areas of life as well.
NURSING SCHOOL STUDY RESOURCES: https://sellfy.com/nursingschoolstudyNURSING
PHARMACOLOGY: https://sellfy.com/p/fnoy/
INSTAGRAM:https://www.instagram.com/your_mentor_rn/?hl=en
PERSONAL INSTAGRAM: https://www.instagram.com/crosby_steen/
MEDIUM ARTICLES: https://medium.com/@rnacademy1..../7-tips-for-nursing-
AMAZON PRIME STUDENT DISCOUNT: https://amzn.to/2OIleAe
VIDEO GEAR
Camera: G7X Markii - https://amzn.to/2na3OR8
Phone: Galaxy Note 8- https://amzn.to/2nboHM3
Audio: Zoom H4NPro Audio Recorder- https://amzn.to/2vktlf8
Computer: 13 inch Macbook Pro- https://amzn.to/2ndhISw
INSTAGRAM TV https://www.instagram.com/crosby_steen/
Hi Guys! My name is Crosby Steen. I am a Nursing Educator, and ER Travel Nurse. I do videos on daily science based news and travel, with the goal of providing value for you in science based education and travel nursing. Any questions hit me up in the comments or Email below.....
PRIVATE TUTORING OR VIDEO REQUESTS CONTACT:
crosby.steen@gmail.com
MUSIC BY: https://andrewapplepie.com/ and copyrighted by Epidemic Sound
Music by Joakim Karud http://youtube.com/joakimkarud
Music by DJ Quads
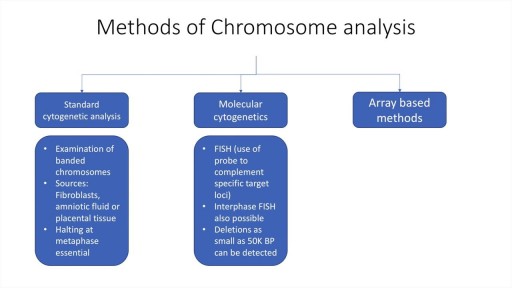
A brief description of the mechanisms, types and assessment of chromosomal analyses. Techniques such as standard cytogenetic testing, FISH and array methods are discussed. Indications for testing in prenatal, neonatal and adult periods are also discussed. Deletions, translocations, inversions etc are described, as are mosaicism and aneuploidy.

Vatche, Minassian, MD, MPH, Chief of Urogynecology, and Sarah Cohen, MD, MPH, Director of the Minimally Invasive Gynecologic Surgery Fellowship Program at Brigham and Women’s Hospital, perform a laparoscopic burch colposuspension, a procedure used to correct stress urinary incontinence.
Stress urinary incontinence is one of the most common types of incontinence and is characterized by urinary leakage during physical activities including coughing, sneezing, exercising, lifting, and laughing. As the condition progresses, it can become severe enough to happen with simple acts such as bending and walking. This condition is due to an anatomic weakness of the bladder neck which typically maintains the seal of urine during activity. Stress incontinence can result from a variety of conditions including vaginal childbirth, aging, menopause and obesity. As this is an anatomic condition, primary treatment may involve pelvic floor exercises and/or minimally invasive surgery.
Learn more about treatment for stress urinary incontinence:
Division of Urogynecology: http://www.brighamandwomens.or....g/Departments_and_Se
Division of Minimally Invasive Gynecologic Surgery: http://www.brighamandwomens.or....g/Departments_and_Se

A Pfannenstiel incision /ˈfɑːnᵻnʃtiːl/ is a type of abdominal surgical incision that allows access to the abdomen. It is used for gynecologic and orthopedics surgeries, and it is the most common method for performing Caesarian sections today.

***SUBSCRIBE WITHIN THE NEXT 28 DAYS FOR A CHANCE TO WIN $1,000!***
Did you know only 20% of our video content is on YouTube? Try out our membership for FREE today! → https://bit.ly/3yRDykI
Try our NCLEX Prep FREE → https://bit.ly/3sRRjvY
Head to https://bit.ly/3yRDykI to get access to the other 80%, along with 800+ study guides, customizable quiz banks with 3,000+ test-prep questions, and answer rationales!
This video illustrates an IM injection for deltoid muscle.
Note that vaccines and other medications can be administered through the deltoid muscle. I will give you some tips through this video.
It is important to check your client’s details such as their medication, time, dose, and the route to be used. Different research works are subject to change the protocols for insertion thus, it is necessary to be up to date with the current changes.
Assemble all the supplies and conduct hand sanitation. Usually, I wear gloves before giving any injection in as much as the CDC may state it is optional unless the patient has an open lesion and contact of body fluids is likely to happen.
Use the acromion process landmark to locate the deltoid muscle. Move your fingers about two widths below the landmark. The patient’s adipose tissue determines the choice of needle length. Note that the needle gauge is determined by the type of medication you plan to give to the patient.
The Z-track technique is recommended rather than pinching the patient’s skin. Pull the patient’s skin to the side using one hand. Use a 90 degree angle to insert the needle to the patient’s skin. At the rate of 10 seconds per mL gently depress the plunger.
Remove the needle carefully and engage the safety precautions then dispose of the needle appropriately in the sharps container. Gauzing helps to cover the injection site.
Nursing School Membership - Try it FREE → https://bit.ly/3yRDykI
New NCLEX Prep - Try it FREE → https://bit.ly/3sRRjvY
Popular Playlists:
NCLEX Fluid & Electrolytes: https://bit.ly/39BSHXs
Heart Failure (CHF): https://bit.ly/2u5zfDm
Myocardial Infarction (MI): https://bit.ly/3bN9AAk
Addison’s vs. Cushing: https://bit.ly/2STvute
Diabetes Mellitus & DKA vs HHNS: https://bit.ly/37D8nbs
Cardiomyopathy: https://bit.ly/38CwcSg
IV Fluids: Hypertonic, Hypotonic & Isotonic: https://bit.ly/2P45BWx
SIADH vs Diabetes Insipidus: https://bit.ly/2wq6Bhb
Follow us on social media for more EXCLUSIVE content 👋
More Videos: https://bit.ly/37CRttH
Instagram: https://www.instagram.com/simplenursing.com_
TikTok: https://www.tiktok.com/simplenursing
Thank you for the support & for tuning in!
Remember… don’t be scared, BE PREPARED!

Screening is looking for cancer before a person has any symptoms. This can help find cancer at an early stage when it may be easier to treat. Lung cancer may have spread by the time a person has symptoms. One reason lung cancer is so serious is because it usually is not found until it has spread and is more difficult to treat. Screening may provide new hope for early detection and treatment of lung cancer. Scientists study screening tests to find those with the fewest risks and most benefits. They look at results over time to see if finding the cancer early decreases a person's chance of dying from the disease.
Today on Crash Course Anatomy & Physiology, Hank breaks down the parts and functions of one of your body's unsung heroes: your epithelial tissue.
Pssst... we made flashcards to help you review the content in this episode! Find them on the free Crash Course App!
Download it here for Apple Devices: https://apple.co/3d4eyZo
Download it here for Android Devices: https://bit.ly/2SrDulJ
Chapters:
Introduction 00:00
Proper Epithelium & Glandular Epithelium 1:38
We're All Just Tubes! 2:12
Cell Shapes: Squamous, Cuboidal, or Columnar 3:34
How Form Relates to Function 4:15
Layering: Simple or Stratified 5:26
Epithelial Cells: Apical & Basal Sides 7:06
Glandular Epithelial Tissue Forms Endocrine & Exocrine Glands 8:20
Review 9:16
Credits 9:54
***
Crash Course is on Patreon! You can support us directly by signing up at http://www.patreon.com/crashcourse
Want to find Crash Course elsewhere on the internet?
Facebook - http://www.facebook.com/YouTubeCrashCourse
Twitter - http://www.twitter.com/TheCrashCourse
Instagram - https://www.instagram.com/thecrashcourse/
CC Kids: http://www.youtube.com/crashcoursekids


In this video, we're going to share 11 things you should NOT do after a tummy tuck. These tips will help you recover from your surgery and keep you from having some common post-tummy-tuck complications. If you're considering a tummy tuck, then be sure to follow these post-operative guidelines!
Dr. William will share all the information you need to make the best decisions for your surgery and recovery. So sit back, relax, and enjoy this video on what NOT to do after an abdominoplasty!
#tummytuck #abdominoplastia #drwilliam
Want a Consultation?
Send us your information: https://drwilliammiami.typefor....m.com/YT-consultatio
Learn more about Dr. William Miami at: https://www.drwilliammiami.com
🔔 Subscribe to our Youtube channel, and stay tuned to all the latest information on cosmetic surgery.
Follow us on Social Media:
Instagram: https://www.instagram.com/drwilliammiami/
Facebook: https://www.facebook.com/Drwilliammiami/
Tiktok: https://www.tiktok.com/@drwilliammiami
OnlyFans: https://onlyfans.com/drwilliammiami
Ogee Recovery: https://ogeerecovery.com
305 Plastic Surgery
564 SW 42nd Ave 3rd floor
Coral Gables, FL 33134
Call us at (305) 209-1030

Eric's Home Dialysis
