- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
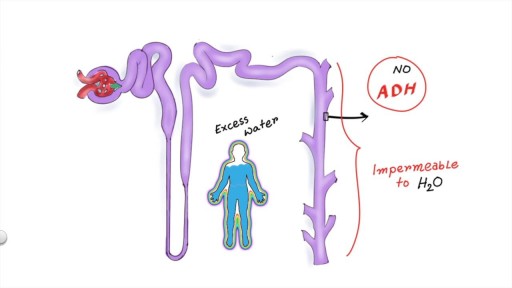
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
http://cfs-cure.plus101.com ----- Chronic Fatigue Syndrome Diet , Cures For Fatigue, Cure For Chronic Fatigue Syndrome. Chronic Fatigue Syndrome Treatment Chronic Fatigue Syndrome (CFS) is variable and unpredictable, and the condition takes its toll on the patient physically, mentally and emotionally. A number of studies have been performed on CFS, with one particular study determining poor early management of the disorder as a primary risk factor for severe CFS. Among the medical community, there is still no consensus on the best course of action for CFS. Most doctors feel that there is no cure for this condition, and limit their treatment to managing the symptoms. There is controversy over different approaches, and main ones being: • Prescription medications • Lifestyle changes • Diet • Nutritional supplements • Graded exercise therapy • Cognitive behavioral therapy • Other alternative/complementary treatments As CFS affects the patients not only physically but also mentally and emotionally, a holistic approach needs to be taken. It is also important that the people around CFS patients understand the condition, and realize that the patient is not just "being lazy" or "constantly feeling down" - chronic fatigue syndrome IS a serious illness and has severe symptoms. Cognitive Behavioral Therapy Cognitive behavioral therapy helps individuals to interpret their symptoms, which in turn helps the patient to shape their behavior in a way to better react to the symptoms. Graded Exercise Therapy A physical therapist can help determine the best exercises for the individual. Programs will start with low levels of exercising, increasing the intensity as the individual gradually builds strength and endurance. Lifestyle Changes Lifestyle changes will also be necessary, including individuals pacing themselves, lowering stress levels, eating a well-balanced diet, engaging in regular moderate exercise, and improving sleep habits. The individual’s work schedule may also need to be modified, as many individuals with CFS find maintaining their regular work schedule too draining. Diet and Chronic Fatigue Syndrome Treatment Diet is crucial in CFS, and dietary supplements may be needed. Certain foods may need to be restricted from the diet, as these may trigger or exacerbate CFS symptoms. A diet-symptom journal can help individuals to identify problem foods. In addition, a significant number of CFS cases may be caused or worsened by un-diagnosed food allergies and intolerances. Therefore, it should be a priority for every patient to check for these using a food-symptom diary and elimination diet, especially if in addition to fatigue you experience gastrointestinal symptoms such as stomach cramps, constipation, or diarrhea. Prescriptions and Medications Depression is often associated with CFS. Antidepressants may be prescribed to treat depression, which in turn will help individuals to cope with CFS-related problems. Studies also show antidepressants administered in low doses may help to relieve pain and improve sleep. Prescription sleep aids may also be prescribed to help individuals improve their sleep. Other drugs that may be prescribed include antiviral drugs, ADD/ADHD medications and anti-anxiety drugs. Alternative/Alternative Chronic Fatigue Syndrome Treatment While the usefulness of alternative/complementary therapy may still be controversial in the scientific community, many patients experience tremendous benefits from these. Main ones include:
Pulsatile Tinnitus Cure, Constant Ear Ringing, Ear Wax Tinnitus, Whistling In Ear, Ringing In Ears. http://tinnitus-solution.info-pro.co First the good news - we know what causes tinnitus. And now the bad news - conventional medical science cannot cure it. Not permanently at least. Sure enough, your doctor would suggest a few remedies, and it may seem to you that the noises you hear are going down. As a result, you begin to relax believing that a pesky problem has been resolved. But suddenly the sounds return again. This is a very common problem actually. So let us turn to the causes instead, and see whether we can try to solve the issue from this end. Here Are Some of the Most Common Causes of Tinnitus Exposure to noise - Did your mom always tell you in your younger days to turn down the volume? She was right. Exposure to loud noise can give you tinnitus. In fact, rock musicians, and those who work with them, or in night clubs often have it. Those who work in construction sites also have tinnitus. So turn down that volume while you still can. You could begin to hear all kinds of noises if you have been exposed to just a single high-pitched noise. Or it could be due to a continuous attack of loud noises close to your ear. This is what happens. Prolonged exposure to noise can damage the Cochlea and cause tinnitus. So if you cannot simply stay away from all that noise, at least get some protection. Use an ear plug when you can. Head injury - Take care of your head because a severe blow or a slight bang could make you hear the tinnitus noises. The head is of course one of the most sensitive parts of the human body. But some people cannot live without an injury, such as those who are into sports - boxers and football players. That's why athletes are more prone to a tinnitus attack. Even a dental surgery could make you hear them. Ear infections and other ear problems - An ear infection, and even sinus can lead to tinnitus as well. When there is an allergy or a sinus infection, the mucous thickens within the inner ear, and this causes more pressure. The extra pressure can lead to tinnitus. Meniere's disease, where the fluid level goes up inside the middle ear is another reason. It could even cause hearing loss. Prescription medications - Conventional drugs often cause side effects, and tinnitus is one of them. Actually, all kinds of drugs have been blamed for instigating this condition. Such as antibiotics like Aminoglycosides, Erythromycin and Vancomycin, Aspirin or medicines containing it. Anti inflammatory drugs like Advil, Aleve, Anaprox, Clinoril, Feldene, Indocin, Lodine and Motrin have also been blamed. Sometimes people heard noises after taking chemotherapy agents such as Cisplatin, Nitrogen Mustard and Vincristine. And some others have even blamed quinine and loop diuretics for this. or even the result of a virus or infection. but is in fact far more shocking that you’ve been led to believe. You’ll finally be able to concentrate on your life, rather that the incessant noise. You’ll be able to no longer live in fear of loud noises, of music, of cinemas. of having fun. The Tinnitus Scandal Revealed, A cure DOES exist. click here: http://tinnitus-solution.info-pro.co
Hidradenitis Suppurativa Surgery, Hidradenitis Suppurativa Photos, Hidradenitis Suppurativa Nz. http://hidradenitis-suppurativa-cure.good-info.co --- symptoms of hidradenitis suppurativa: First let us look at the symptoms of the disease Black heads: When they appear in a double barreled pattern Red bumps: When tender lesions, or bumps, which often contain pus and/or itching. Hard, painful lumps: When pea sized lumps cause pain and get inflamed These recur very often Don’t heal or improve for weeks Returns after treatment Appears in several different locations The lumps are accompanied by pain I am going to reveal to you step by step how to understand and deal with the problems of hidradenitis suppurativa. click here http://hidradenitis-suppurativa-cure.good-info.co

Watch that Huge Stomach Tumor Removal Medical Surgery

Watch that World's first osteotomy surgery for spine deformity

Como Aumentar La Testosterona, Testosterona Masculina, Como Aumentar El Nivel De Testosterona --- http://aumentar-testosterona.good-info.co/ --- ¿Baja Testosterona En Hombres Es Peligrosa? ¿Cual es la hormona en los hombres que les permite construir músculo magro, quemar más grasa, ser más fertíil y aumentar la energía de manera general? es la TESTOSTERONA La testosterona es una hormona tan esencial para los hombres porque en realidad define lo que es la virilidad masculina. Y la pérdida de esta hormona tan importante resulta en: * Aumentos de peso * Falta de deseo * Falta de energía y motivación * Pérdida de músculo magro * Depresión * Grasa de pecho Lo que sucede hoy en dia es que más hombres que nunca están perdiendo la testosterona. De hecho, segun el famoso (experto de hormonas masculinas) el nivel de testosterona en los hombres disminuye tan rapidamente que es una verdadera CRISIS para los hombres. Si tu o otra persona experimenta la baja testosterona que sepa que NO es por tu culpa! ¿Cansado Con Tus Bajos Niveles De Testosterona, Tu Sobrepeso y Tu Falta de Libido? Haga click aqui http://aumentar-testosterona.good-info.co/

Verrugas En El Cuello, Como Borrar Lunares De La Cara, Como Quitar Las Verrugas Del Cuello --- http://sinverrugasylunares.plus101.com --- El Ajo Para Eliminar Las Verrugas, PRUEBALO!!! Antes que nada déjame comentarte que el ajo es un poderoso antiséptico, con propiedades fungicidas, bactericidas y también ayudan a depurar nuestro cuerpo. El ajo es rico en un compuesto llamado alicina, este elemento es un poderoso antivirus y anti bacterial natural, eso sin mencionar las propiedades antioxidantes que el ajo posee las cuales son de enorme beneficio para la salud de nuestra piel y por supuesto la salud en general. Es un tratamiento sencillo pero bastante efectivo, te recomiendo que lo comiences a partir de hoy mismo. Por las mañanas en ayunas tomate un ajo crudo, esto con el fin de limpiar nuestro organismo de virus y bacterias. Recuerda que nuestra misión es eliminar la raíz de las verrugas y los lunares tal como lo hablamos anteriormente el responsable de las verrugas es el virus del papiloma humano. El ajo gracias a sus propiedades antivirales nos ayudarán a combatir el virus desde adentro. Haz esto todos los días. Tomándote un ajo diario en ayunas estarás atacando el virus desde adentro, Ahora lo atacaremos desde fuera Para esto necesitarás un ajo, debes partirlo en porciones pequeñas calcula el tamaño de las porciones para cubrir los lunares y/o tus verrugas. Y ahora da a conocer el mismo método que él utilizó para curarse y eliminar las verrugas y lunares para siempre. Te invito a conocerlo a través del siguiente enlace: http://sinverrugasylunares.plus101.com

Tummy tuck surgery, also known as abdominoplasty, removes excess fat and skin and, in most cases, restores weakened or separated muscles creating an abdominal profile that is smoother and firmer. A flat and well-toned abdomen is something many of us strive for through exercise and weight control. Sometimes these methods cannot achieve our goals. Even individuals of otherwise normal body weight and proportion can develop an abdomen that protrudes or is loose and sagging. The most common causes of this include: Aging Heredity Pregnancy Prior surgery Significant fluctuations in weight What tummy tuck surgery can't do A tummy tuck is not a substitute for weight loss or an appropriate exercise program. Although the results of a tummy tuck are technically permanent, the positive outcome can be greatly diminished by significant fluctuations in your weight. For this reason, individuals who are planning substantial weight loss or women who may be considering future pregnancies would be advised to postpone a tummy tuck. A tummy tuck cannot correct stretch marks, although these may be removed or somewhat improved if they are located on the areas of excess skin that will be excised.

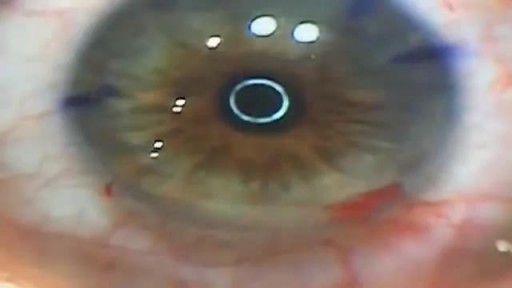
cleral tattooing is the practice of tattooing the sclera, or white part of the human eye. The dye is not injected into the tissue, but between two layers of the eye, where it spreads out over a large area. The process is not common
Like a fine whiskey barrel and wine cellar, cannabis also comes at its best when aged in a dark, cool place. Though there is no steadfast expiration date for cannabis, the method you use for preserving the cannabis makes a big difference in maintaining the buds’ freshness and potency. The question is, how do you store cannabis in a way that could extend its longevity while maintaining the vigor and freshness? Experts have described different methods. However, here are some time-proven methods that are easy and inexpensive and require very less equipment. Use air-tight glass containers to store the weed Use clean air-tight glass containers or jars to store cannabis. You can buy glass containers from any ordinary supermarket or hardware store. The tricky part is to make sure you do leave some air in the container while the air stored with cannabis isn’t in detrimental extent. Always leave 1/4 space at the top of the canister or container. Do not fill the containers to the brim with the buds. If you leave no air, then the buds will dry out. If you have too much air, the buds will get damp and moldy. Freeze your cannabis in a convenient temperature The best way to store your buds is in air-tight glass jars, in a cool and dark place under an ideal temperature between 60 and 70 degrees Fahrenheit. If you need to store a high volume of cannabis, you can freeze them after keeping them completely dry for a period of 4 weeks. On this note, you should know that you must not handle frozen buds until it becomes normal in room temperature as trichomes become brittle and can easily break off in freezing temperature. Refrigerate your cannabis (Not Recommended) Even if you use airtight jars, cannabis can grow mold in the fridge. So, you should avoid storing cannabis in the fridge. If you can’t help but doing it, make sure the weed is completely dry and put them in the back where the humidity and temperature don’t fluctuate. Plastic Baggies (Worst method!) Albeit this is very common among people who aren’t expert in handling cannabis, this is the worst of all storage methods. Cannabis gets brittle and dries out in plastic bags. It also loses its natural smell, and the potency deteriorates sharply. So, it should be avoided entirely or can be used for a short-term if there is no better alternative. Here are some things you should know while storing cannabis - Make sure cannabis has been cured for at least 4 weeks before putting them into long-term storage. Without proper curing before storage, the buds can lose their strength and smoothness. - Sunlight can stop the medicinal qualities of cannabis. Your cannabis, if stored correctly, can maintain its medicinal qualities for a few years. Exposure to Sun will turn your cannabis brown, no matter how you have stored it away. - Air-tight, nonporous glass jar are the best way for storing the buds for long term. You can use metal or plastic box/bag, but that could reduce the smell and taste after a while. - Avoid heat and middling temperature in the place where you store your buds. The ideal temperature is 60-70°F (15-21°C) or under 32°F (0°C). Extra heat, cold or middling temperature cause the cannabis potency to decrease. - Keep your cannabis away from any electronic devices or appliances that will expose the cannabis to heat. Keeping cannabis on top of a microwave, or near a laptop or mobile charge is a bad idea. Now, as you know that how to store cannabis properly and make it last for years, enjoy the best form of your weeds even it comes from the previous year. Do write to us in the comments section if you have any questions. Also, don’t forget to hit the subscribe button below. Visit OnlineMedicalCard.com now to get an MMJ recommendation online in less than 10 minutes.

Buy Natural Certified Original Gem stones, Rashi based gemes stone, Semi-Precious-Stone, Pooja Article Like Sulemani Hakik, Onyx, Ruby, Manik, Hakik, Amethyst, Pukhraj, Neelam, Panna, Gomed, Moti, Moonga, Manik, Cat'seye, Citrine, Lajaward, Moonstone. Topaz, Yemeni, etc. You can also buy yantra line Shree Yantra, Parad, Etc. This Ramzan celebrates with Certified Original Sulemani Hakik Stone.
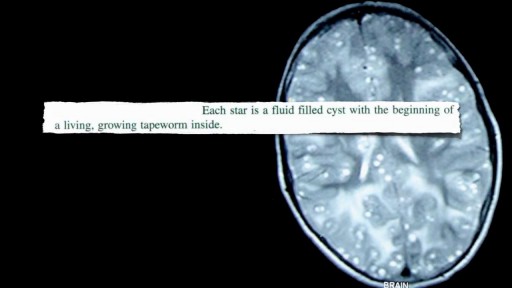
Neurocysticercosis Pork Worms Infecting Human Brain

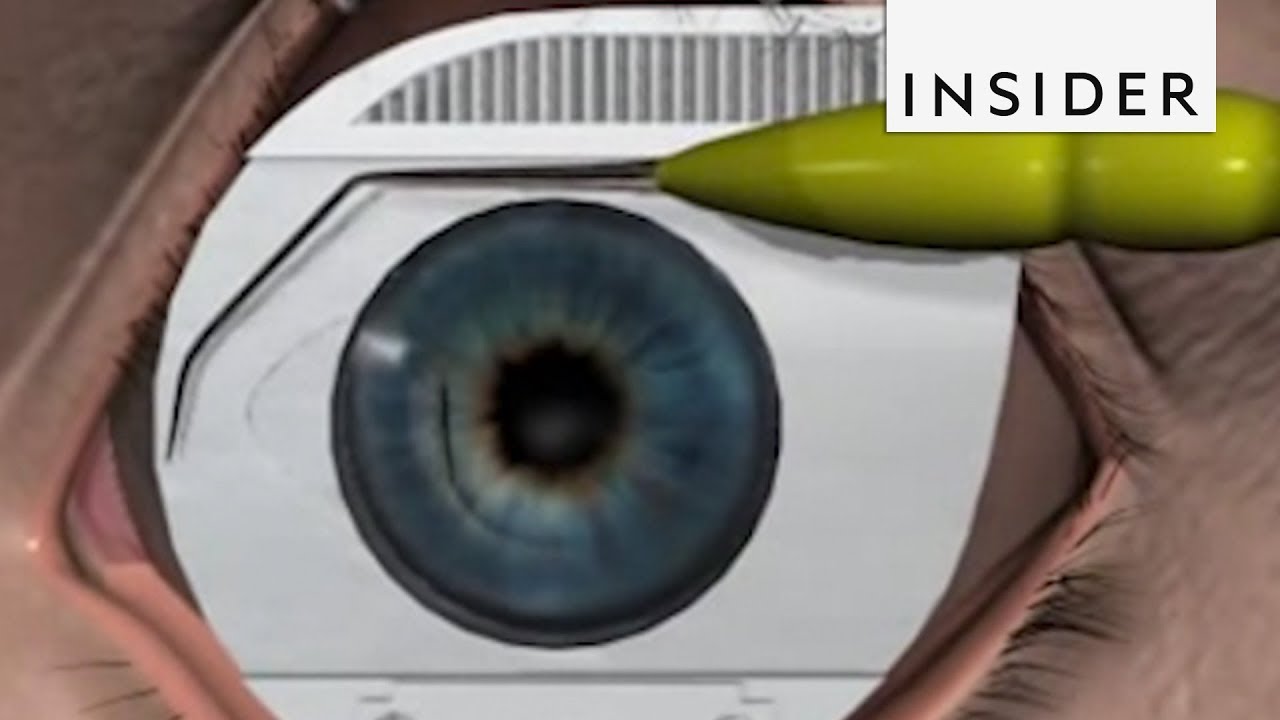
Here’s how surgeons perform LASIK surgery.
See more: https://www.amerra.com/
Subscribe to our new channel, INSIDER food: http://insder.co/2kWwBKZ
The INSIDER team believes that life is an adventure! Subscribe to our channel and visit us at: https://thisisinsider.com
INSIDER on Facebook: https://www.facebook.com/thisisinsider/
INSIDER on Instagram: https://www.instagram.com/thisisinsider/
INSIDER on Twitter: https://twitter.com/thisisinsider

Examination of the hand and the wrist

A video showing the PRK laser eye surgery
How to apply and safely remove a plaster cast
