- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Endometrial Polyp is removed using a IUR (Smith@Nephew)by B.C. Schoot Gynaecologist dept OB/GYN Catharina Hospital Eindhoven The Netherlands
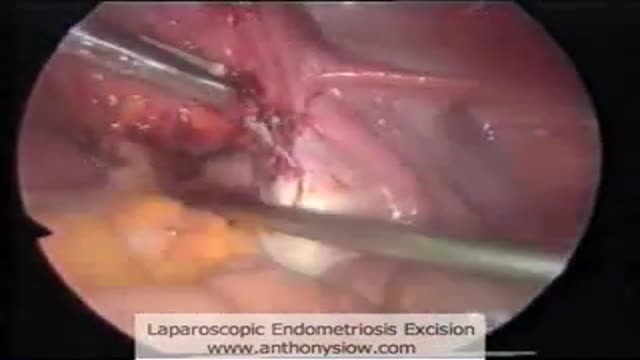
Laparoscopic excision of endometriosis

David Beckham Medical Exam

Examination of varicose veins

Video shows a fine needle biopsy with guided ultrasound of a thyroid nodule.

A video showing how to perform Cardio-Pulmonary Resuscitation on a child

An Emergency Medicine video showing how to perform Jaw Thrust technique
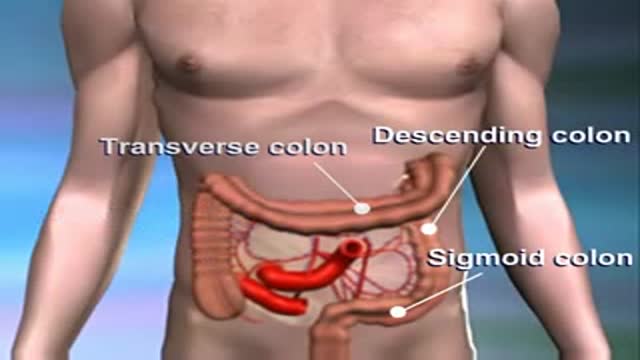
An animation illustrating carcinoma of the colon

Basic Surgical Instruments- Forceps, scissors.

Endoscope-assisted pocket grafting of autologous collagen for correction of facial wrinkles

Better Vein Care and Safer Injection
Loyola Full Thorax Exam Part 2 A video from Loyola Medical School, Chicago showing the medical and clinical examination of the respiratory system.

Scalpel Holding and Cutting

Use of Skin Stapler Remover

Esophagomyotomy for Achalasia

closing up teeth spaces

Choking Infant Video Demonstration

Laparoscopic Sleeve Gastrectomy

The back part of the upper jaw has the highest failure rate abotu 20% overall due to the presence of the sinus and the soft quality of bone.

At Hutzel Women's Hospital, Dr. Giancarlo Mari performs breakthrough in-utero surgery to save the lives of high-risk twins developing with a rare "shared" circulatory problem. ~ Detroit Medical Center
