- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

You can see more videos on ENT channel.
Tampa body sculpting is the specialty of Dr. Thomas Su of the Artistic Lipo Sculpting Center. Dr. Su’s dedication to body contouring has allowed him to finely hone his craft over the years, making him the most trusted Tampa lipo surgeon. To learn more about Tampa fat removal procedures, visit http://www.artlipo.com/liposuction/liposuction-body-areas/lipo-abdomen.html.
Fundoplication HD GERD Surgery 3D Animation

Robotic Prostatectomy Cornell Athermal Robotic Technique
Histology of Tongue
Histology of Tongue Folliate Papilla
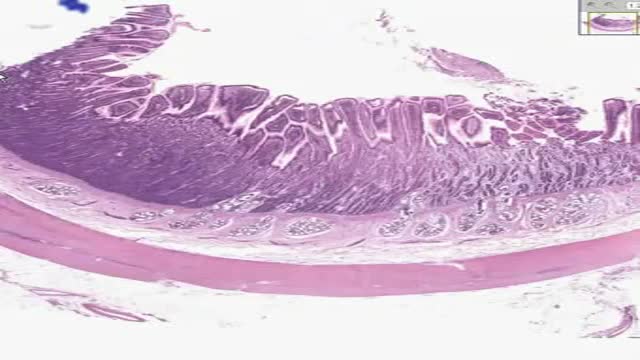
Histology of Small Intestine Duodenum
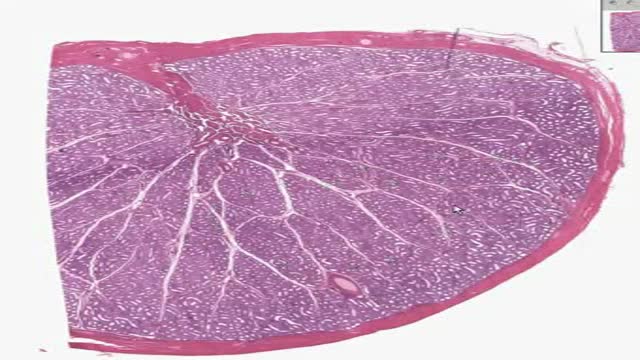
Histology of Testis
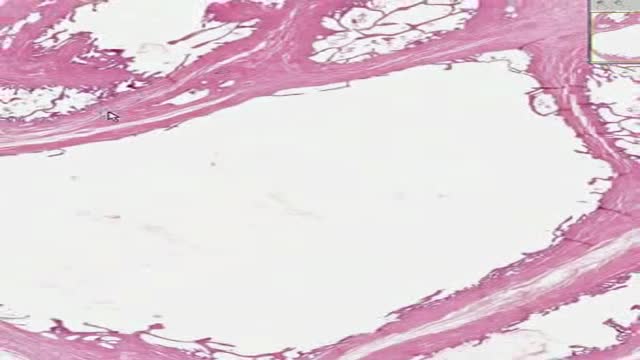
Histology of Seminal Vescicles

breast augmentation-breast implants
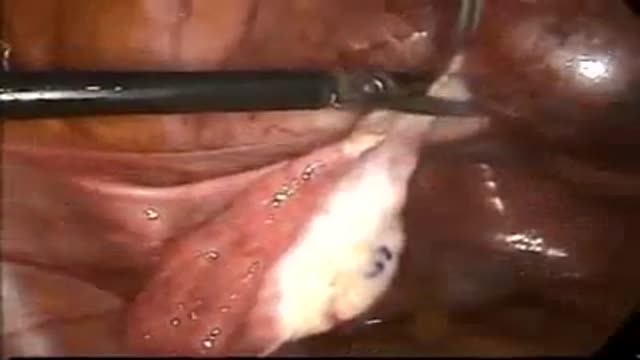
Ectopic Pregnancy in left Cornu Laparoscopic Surgery

Male 19 y. age victim of penetrating brain injury. All the criteria for the encephalic death diagnosis were present. The presence of this complex spinal reflex doesn't exclude the brain death diagnosis and must be known and understood by the professionals involved in this very important diagnosis

AirXpanders Inc. designs, manufactures and distributes the revolutionary AeroFormTM Patient Controlled Tissue Expander. A first for women who choose reconstructive surgery following a mastectomy, the AeroForm tissue expander does not use intrusive and painful saline injections via syringe needles. The AeroForm patient controlled tissue expander utilizes a needle-free inflation system via a patient-controlled handheld device, which releases specified amounts of air in the form of carbon dioxide

Best facial cosmetic surgeons Best facial plastic surgeon Browlift Charlotte endoscopic brow lift Charlotte’s top facial plastic surgeon Facial plastic surgeons Facial plastic surgery Face lifts Facial mini-tuck Lip enhancement Lip augmentation Nose j

men health,women health,organ devloping ,female problems soultion,

The term chronic inflammatory demyelinating polyradiculoneuropathy (CIDP) has been used to identify patients with a chronically progressive or relapsing symmetric sensorimotor disorder with cytoalbuminologic dissociation and interstitial and perivascular endoneurial infiltration by lymphocytes and macrophages. It can be considered the chronic equivalent of acute inflammatory demyelinating polyradiculoneuropathy, the most common form of Guillain-Barré syndrome. Signs and symptoms CIDP typically starts insidiously and evolves slowly, in either a slowly progressive or a relapsing manner, with partial or complete recovery between recurrences; periods of worsening and improvement usually last weeks or months. Most experts consider the necessary duration of symptoms to be greater than 8 weeks for the diagnosis of CIDP to be made. Symptoms reported include the following: Preceding infection (infrequent) Initial limb weakness, both proximal and distal Sensory symptoms (eg, tingling and numbness of hands and feet) Motor symptoms (usually predominant) In about 16% of patients, a relatively acute or subacute onset of symptoms In children, usually a more precipitous onset of symptoms Symptoms of autonomic system dysfunction (eg, orthostatic dizziness) Pertinent physical findings are limited to the nervous system, except when the condition is associated with other diseases. Such findings may include the following. Signs of cranial nerve (CN) involvement (eg, facial muscle paralysis or diplopia) Gait abnormalities Motor deficits (eg, symmetric weakness of both proximal and distal muscles in upper and lower extremities) Diminished or absent deep tendon reflexes Sensory deficits (typically in stocking-glove distribution) Impaired coordination See Clinical Presentation for more detail. Diagnosis Laboratory studies that may be helpful include the following: Cerebrospinal fluid analysis: Elevated protein levels are common (80% of patients); 10% of patients also have mild lymphocytic pleocytosis and increased gamma globulin Complete blood count (CBC), erythrocyte sedimentation rate (ESR), antinuclear antibody (ANA) level, biochemistry profile, and serum and urine immunoelectrophoresis (to exclude associated systemic disorders) In certain instances, genetic testing Other tests and procedures that may be warranted are as follows: MRI of the spine with gadolinium enhancement Electromyography (EMG) is a critical test to determine whether the disorder is truly a peripheral neuropathy and whether the neuropathy is demyelinating Peripheral (sural) nerve biopsy (see the image below): This is considered when the diagnosis is not completely clear, when other causes cannot be excluded, or when profound axonal involvement is observed on EMG; biopsy was once commonly recommended for most patients before immunosuppressive therapy, but current guidelines no longer recommend it

penetrating neck trauma case
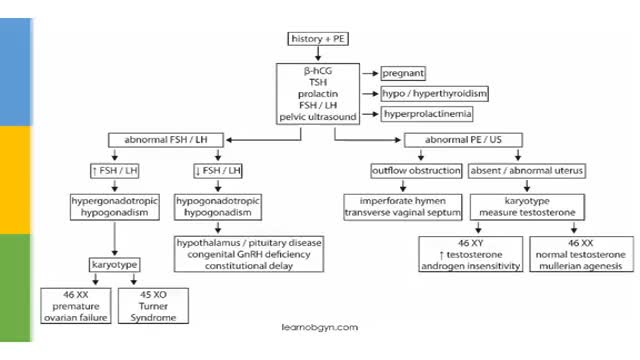
Amenorrhea is the absence of menstrual bleeding.[1] Amenorrhea is a normal feature in prepubertal, pregnant, and postmenopausal females. In females of reproductive age, diagnosing amenorrhea is a matter of first determining whether pregnancy is the etiology. In the absence of pregnancy, the challenge is to determine the exact cause of absent menses.[2] Primary amenorrhea is the failure of menses to occur by age 16 years, in the presence of normal growth and secondary sexual characteristics. If by age 13 menses has not occurred and the onset of puberty, such as breast development, is absent, a workup for primary amenorrhea should start. Secondary amenorrhea is defined as the cessation of menses sometime after menarche has occurred. Oligomenorrhea is defined as menses occurring at intervals longer than 35 days apart. No consensus has been reached regarding the point at which oligomenorrhea becomes amenorrhea. Some authors suggest the absence of menses for 6 months constitutes amenorrhea, but the basis for this recommendation is unclear. For a post-menarchal girl or a reproductive-aged woman to experience a menstrual cycle interval of more than 90 days is statistically unusual. Practically speaking, this should be an indication for an evaluation to seek the cause.

Pulmonary surfactant is a mixture of lipids and proteins that is produced by alveolar type II epithelial cells (AEC2) and secreted into the airspaces. Phospholipids are the major component of surfactant by weight, and are essential for lowering surface tension at the air-liquid interface, which prevents alveolar collapse at end-expiration. Four proteins highly expressed in the lung and found in surfactant are designated surfactant proteins (SP) A, B, C, and D. Additional proteins including ABCA3 and NKX2.1 are also important for the production of functional surfactant. The surfactant proteins are developmentally regulated, such that their expression increases in later gestation

Yeast Infection Symptoms in Women and Men - Causes, Signs, photos, Pictures of Candidiasis Fungus
