- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Extremely funny, and very in-depth look at all the parts and pieces of your blood.

Every year, thousands of conventional total shoulder replacements are successfully done in the United States for patients with shoulder arthritis. This type of surgery, however, is not as beneficial for patients with large rotator cuff tears who have developed a complex type of shoulder arthritis called "cuff tear arthropathy." For these patients, conventional total shoulder replacement may result in pain and limited motion, and reverse total shoulder replacement is a better option.

Medial medullary syndrome, also known as Dejerine syndrome, represents less than 1% of brainstem stroke syndromes. Thrombotic or embolic occlusion of small perforating branches from vertebral or proximal basilar artery supplying the medial aspect of medulla oblongata cause this rare syndrome. It is characterized by contralateral hemiplegia/hemiparesis as well as hemisensory loss with ipsilateral hypoglossal palsy (ipsilateral tongue weakness and atrophy) from involvement of CN XII nucleus. Other manifestations e.g. vertigo, nausea, ipsilateral limb ataxia are also reported.

Lasic in 10 years old girl for Myopia
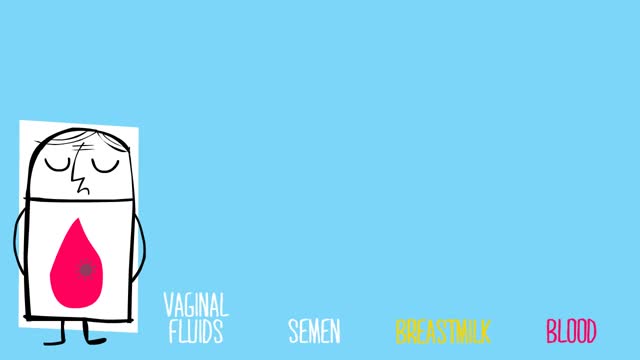
-Almost all the cases of occupational transmission of HIV have been due to transmission via exposure to blood and certain body fluids. The body fluids wherein standard precautions have been recommended include semen, vaginal secretions, and any other body fluid containing visible blood. Other standard precautions, according to the Center for Disease Control and Prevention (CDC), also apply to cerebrospinal, peritoneal, pleural, pericardia!, synovial fluid, or any other tissue, even though the epidemiologic data regarding the risk of HIV transmission from these fluids is insufficient. Standard precautions do not apply to urine, sweat, tears, sputum, vomitus, and nasal secretions or feces, as long as there is no gross visible blood. The occupational transmission of HIV has never been documented from the above sources.

The clinician performing the procedure should be familiar with the anatomy of the specific joint and cognizant of the relevant landmarks in order to avoid puncture of tendons, blood vessels, and nerves (see the images below).
Multiple myeloma is a cancer formed by malignant plasma cells. Normal plasma cells are found in the bone marrow and are an important part of the immune system. The immune system is made up of several types of cells that work together to fight infections and other diseases. Lymphocytes (lymph cells) are the main cell type of the immune system. The major types of lymphocytes are T cells and B cells.

Squamous cell carcinomas typically appear as persistent, thick, rough, scaly patches that can bleed if bumped, scratched or scraped. They often look like warts and sometimes appear as open sores with a raised border and a crusted surface. In addition to the signs of SCC shown here, any change in a preexisting skin growth, such as an open sore that fails to heal, or the development of a new growth, should prompt an immediate visit to a physician.

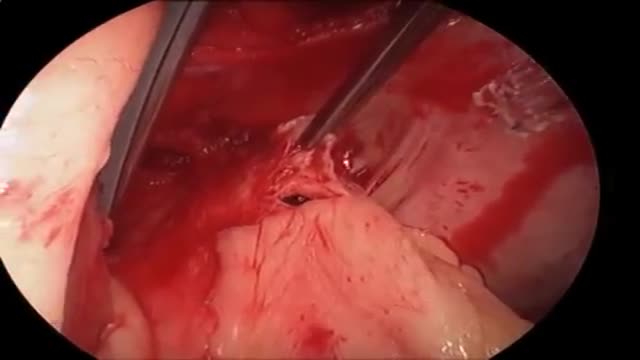
At first, grasping the needle is difficult because it will have a tendency to want to jump around. What can oftentimes help is to get hold of the thread with the left-hand forceps at a point 2 to 3 cm away from the needle. Dangle the needle until it just comes to rest on the surface. This will then allow you to use the angulated needle holder to grab the needle easily. Your needle is in a stable position if it is set up to 90 degrees to the axis of the tips of the forceps. You can make minor corrections by touching the needle with your left-hand forceps, or by partially relaxing your grip and nudging the needle tip against another firm object. You should hold the needle just behind its midpoint (If you hold it too near the tip, it will point downward. If you hold it too near the thread end, it will point upward.).
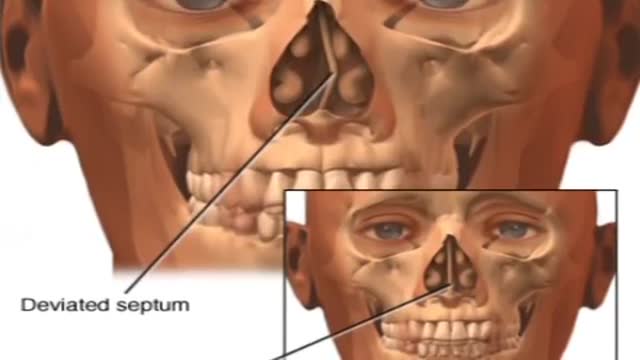
Nosebleeds are common. Most often they are a nuisance and not a true medical problem. But they can be both. Nosebleed care Sit upright and lean forward. By remaining upright, you reduce blood pressure in the veins of your nose. This discourages further bleeding. Sitting forward will help you avoid swallowing blood, which can irritate your stomach. Pinch your nose. Use your thumb and index finger to pinch your nostrils shut. Breathe through your mouth. Continue to pinch for five to 10 minutes. Pinching sends pressure to the bleeding point on the nasal septum and often stops the flow of blood. To prevent re-bleeding, don't pick or blow your nose and don't bend down for several hours after the bleeding episode. During this time remember to keep your head higher than the level of your heart. If re-bleeding occurs, blow out forcefully to clear your nose of blood clots and spray both sides of your nose with a decongestant nasal spray containing oxymetazoline (Afrin, Mucinex Moisture Smart, others). Pinch your nose again as described above and call your doctor. When to seek emergency care The bleeding lasts for more than 20 minutes The nosebleed follows an accident, a fall or an injury to your head, including a punch in the face that may have broken your nose
Your lungs are have 600 million air pockets -- enough to cover a tennis court.
Scientists are working on a pill that could replace exercise.
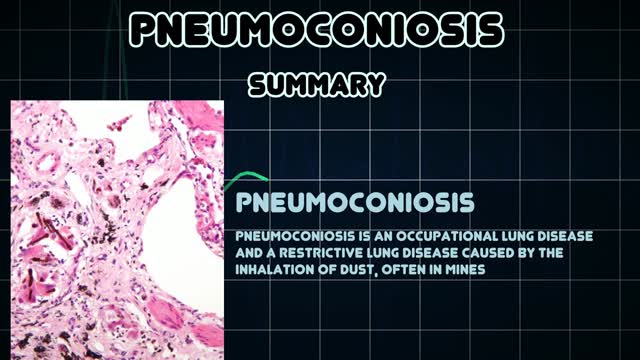
Pneumoconiosis is a general term given to any lung disease caused by dusts that are breathed in and then deposited deep in the lungs causing damage. Pneumoconiosis is usually considered an occupational lung disease, and includes asbestosis, silicosis and coal workers' pneumoconiosis (CWP), also known as "Black Lung Disease."
Pulmonary embolism symptoms can vary greatly, depending on how much of your lung is involved, the size of the clots, and whether you have underlying lung or heart disease. Common signs and symptoms include: Shortness of breath. This symptom typically appears suddenly and always gets worse with exertion. Chest pain. You may feel like you're having a heart attack. The pain may become worse when you breathe deeply (pleurisy), cough, eat, bend or stoop. The pain will get worse with exertion but won't go away when you rest. Cough. The cough may produce bloody or blood-streaked sputum. Other signs and symptoms that can occur with pulmonary embolism include: Leg pain or swelling, or both, usually in the calf Clammy or discolored skin (cyanosis) Fever Excessive sweating Rapid or irregular heartbeat Lightheadedness or dizziness
People with lactose intolerance are unable to fully digest the sugar (lactose) in milk. As a result, they have diarrhea, gas and bloating after eating or drinking dairy products. The condition, which is also called lactose malabsorption, is usually harmless, but its symptoms can be uncomfortable. A deficiency of lactase — an enzyme produced in your small intestine — is usually responsible for lactose intolerance. Many people have low levels of lactase but are able to digest milk products without problems. If you're actually lactose intolerant, though, your lactase deficiency leads to symptoms after you eat dairy foods.

Pediatric 4-Step Basic Technique
The pathobiology of MM is complex and the root underlying cause of myeloma is the multistep genetic changes in the postgerminal center B cell. In addition, the bone marrow microenvironment plays a crucial role.[2] The interaction between myeloma cells and the microenvironment is mediated through adhesive interactions via cell-surface receptors, paracrine loops involving several cytokines, such as IL-6, VEGF and IL-10, and suppression of cell-mediated immunity.[2–4] IMiDs modulate many of these interactions leading to decreased myeloma cell growth and survival. Thalidomide was the first IMiD introduced to treat MM. It was initially synthesized in Germany in the late 1950s to treat insomnia and morning sickness. It was withdrawn from the market in 1961 because of its teratogenic effects. Its immunomodulatory properties were realized when it was observed to improve erythema nodosum leprosum, a painful immunologic reaction of leprosy, leading to its approval by the FDA in 1998 with tight prescribing and marketing regulations. Subsequent research showed the diverse mechanism of action of thalidomide including its immunomodulatory effect by inhibition of de novo IgM antibody synthesis,[5] modulation of the T-cell subset by increasing the T-helper cells, inhibitory effects on the TNF-α and antiangiogenic activity leading to its use in MM. Significantly higher response rates in combination with dexamethasone led to its approval in the treatment of newly diagnosed MM in 2006. Lenalidomide, a second-generation IMiD, was developed from the structural backbone of the thalidomide molecule by the addition of an amino group (NH2-) at position 4 of the phthaloyl ring and removal of the carbonyl group (C = O) of the 4-amino-substituted phthaloyl ring (Table 1).[6] In addition to immunomodulatory effects, other mechanisms of action have been described such as direct cytotoxicity via induction of apoptosis, inhibition of cell adhesion molecules and inhibition of growth signals that promote bone marrow angiogenesis

What combines research opportunities, intellectual challenge, and international collaboration in the study of a disease which affects many organs of the body and all sectors of society? And demands that specialists from many different backgrounds work together to crack sometimes intractable problems? It is, of course, oncology. As a career choice, it's demanding; it takes passion coupled with a willingness to put in the hours and to learn how to discuss death honestly and sensitively. But for the right person, it can be immensely rewarding.

