- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Risks & Benefits of Epilepsy Surgery | Epilepsy

This tiny camera can capture images inside the brain.

#STOP VIOLENCE AGAINST DOCTORS#SAVE THE DOCTOR
Despite the effective diagnostic and treatment options available today, Dr. Wolfe notes that he continues to see a high number of untreated scaphoid fractures that have progressed to nonunion. However, he adds that this may not be the result of a missed diagnosis, but rather more related to the relatively innocuous injury that causes a low level of suspicion. Recognition and awareness of scaphoid fractures is higher today among primary care providers, emergency room physicians, pediatricians, and sports trainers, but fully 15% of patients with suggestive physical findings and normal initial x-rays will have an “occult”, or concealed, scaphoid fracture. Specialized imaging studies are critical at an early stage to reduce the chance of scaphoid nonunion.
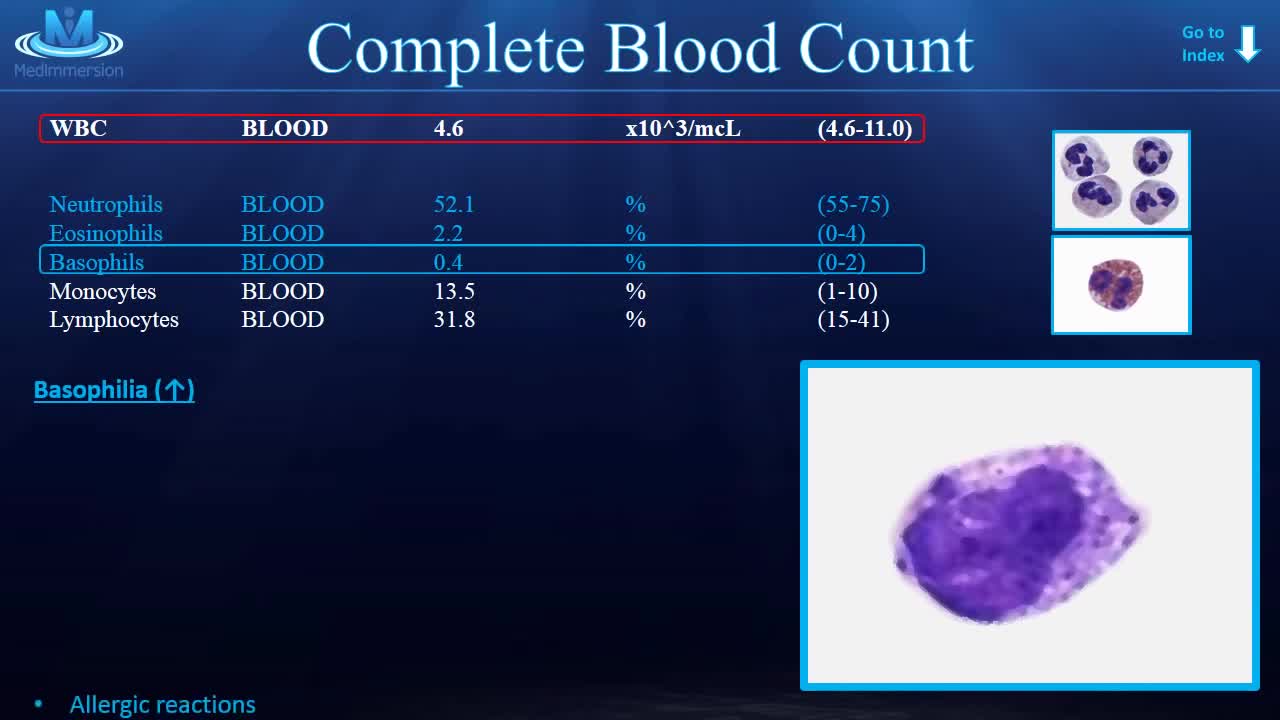
Learn the CBC once and for all!
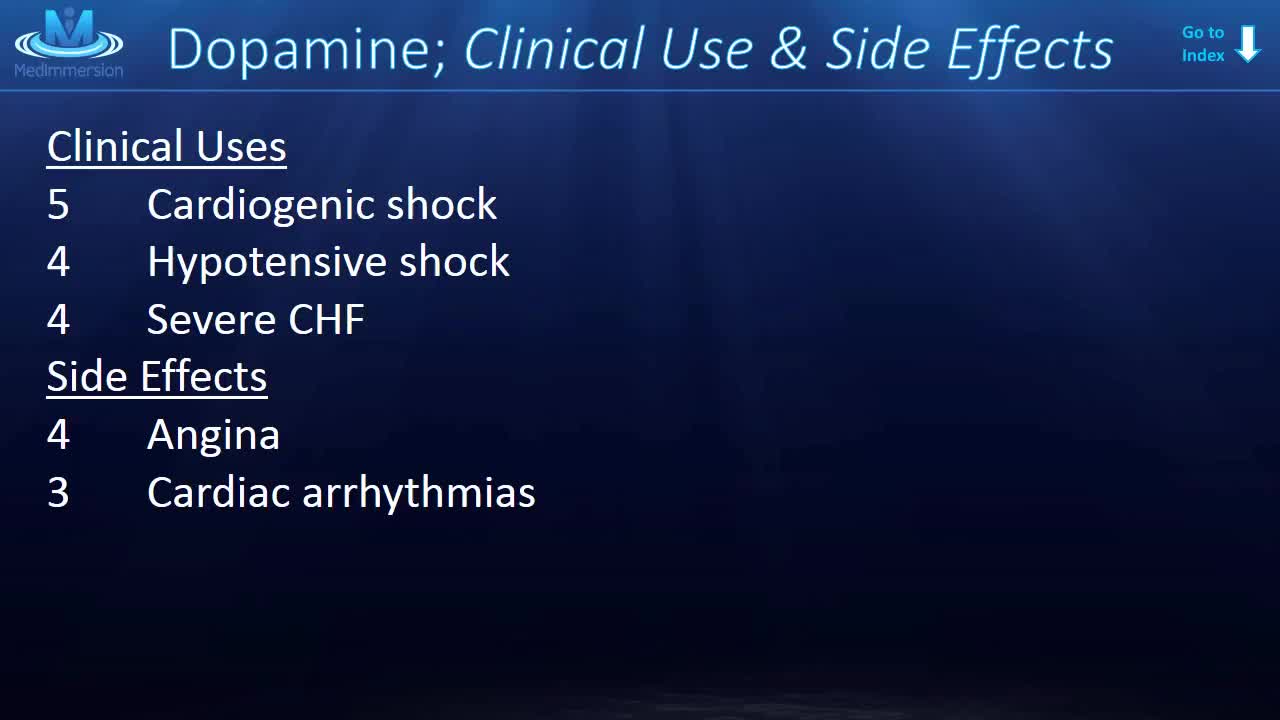
Dopamine is the one neurotransmitter that everyone seems to know about. Vaughn Bell once called it the Kim Kardashian of molecules, but I don’t think that’s fair to dopamine. Suffice it to say, dopamine’s big. And every week or so, you’ll see a new article come out all about dopamine.
Every owner of a building where asbestos abatement activity occurs is responsible for the performance of the asbestos abatement activities by his/her agent, contractor, employee, or other representative. Each building owner is responsible for determining the amount of asbestos-containing material that may be disturbed during the course of work. The size and scope of the overall project, with particular reference to the total amount of asbestos-containing material that will be disturbed determines the reporting or filing requirements established in the Asbestos Control Program Rules. An asbestos project is defined as any form of work that will disturb more than 25 linear feet or more than 10 square feet of asbestos-containing material.

Intraarticular Fracture Base of Thumb Metacarpal Surgery
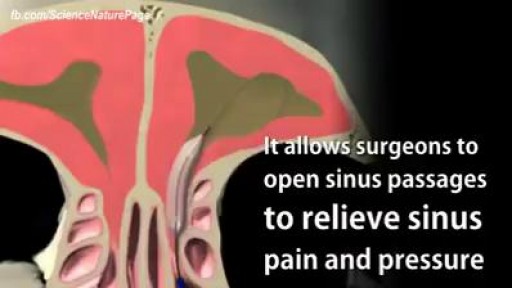
Balloon Sinuplasty for Sinus Infection

Meckel's Diverticulum is a vestigeal remnant of vitellointestinal duct. Its a true diverticulum as it contains all three layers of intestine. It is usually presents at anti mesenteric burder. Usually 2 cm (range 1- 12 cm ) in length, found in 2 % of population , and situated around 2 feet of Ileaocecal junction. 50 % cases it contains gastric mucosa , but may also contain colonic, duodenal or pancreatic mucosa .male : female ration in symptomatic cases is 3 : 1.It may mimic acute appendicitis, so in cases where one is going for surgery for appendicitis , must search for meckel's diverticulum........

Open appendectomy (simulated)

Watch that video for a Boy Returns from the Beach with a Snail Inside His Knee

Watch that video of a Man Impaled by Shovel In His Butt Inside ER

Transcript: Body Restoration (http://stalbertphysiotherapy.com/) has treated over 12,400 patients since it opened its doors in 1992. While embracing new technology and techniques they have not left behind the basic tenets of hands-on healing. If you are injured or have chronic pain, the mission is to help you live pain-free. Relief is a click or a phone call away. Come in for your no obligation exam and find out what will work for you.
Come Si Può Rimanere Incinta, Rimanere Incinta A 42 Anni Naturalmente, Settimane Di Gravidanza--- http://come-rimanere-incinta.info-pro.co --- Come rimanere incinta in modo naturale La sterilità può essere generalmente definita come l'incapacità di avere una gravidanza dopo aver provato per almeno un anno senza l'uso di contraccettivi. Nei paesi occidentali la sterilità colpisce circa il 15% della popolazione. Mentre c'è chi cerca di concepire con metodi alternativi come la fecondazione in vitro, altri preferiscono ottimizzare le probabilità di rimanere incinta naturalmente. Cercare di rimanere incinta naturalmente può essere molto importante dal momento che molte coppie o individui con diagnosi di sterilità possono tornare ad essere fertili senza trattamenti (e quindi si dovrebbe parlare di "sub-fertilità" piuttosto che di "sterilità"). Quando si cerca di rimanere incinta naturalmente, il fattore più importante è capire il ciclo mestruale e la tempistica di ovulazione, che porta ad ottimizzare le possibilità di ottenere una gravidanza. Di solito l'ovulazione avviene intorno al quattordicesimo giorno e, di conseguenza, per ottenere una gravidanza naturale la coppia dovrebbe avere più rapporti sessuali possibili tra il dodicesimo e il quindicesimo giorno. Ogni donna ha un ciclo leggermente diverso. Per cui, per migliorare le probabilità di rimanere incinta, è indispensabile studiare i propri cicli e calcolare con esattezza quando si ovula. L'antico Sistema Olistico Cinese In 5-passi Per Rimanere Incita Naturalmente E Avere Bimbi Sani Clicca sul link http://come-rimanere-incinta.info-pro.co

Watch that video to know How to Treat Pimples on Your Face?

Draining a Blood Clot from the left thigh after knife stab wound sutured by some ER!



NEW WAVE Surgical Technique 3D Animation
