- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Prosthetic Aortic Valve Replacement Surgery 3D
Respiratory System Structure and Functions
Removal of rupture appendix
For the elderly, consuming a healthy diet is important to maintaining a strong body and increasing longevity. Many seniors can suffer from vitamin D deficiency due to a lack of exposure to sunlight and by avoiding certain foods. Without enough vitamin D, there are several effects that it can have on both the body and mind for those who are over the age of 50.
http://www.homecareassistancechicago.com/

Middle cerebral artery syndrome is a condition whereby the blood supply from the middle cerebral artery (MCA) is restricted, leading to a reduction of the function of the portions of the brain supplied by that vessel: the lateral aspects of frontal, temporal and parietal lobes, the corona radiata, globus pallidus, caudate and putamen. The MCA is the most common site for the occurrence of ischemic stroke.[1] Depending upon the location and severity of the occlusion, signs and symptoms may vary within the population affected with MCA syndrome. More distal blockages tend to produce milder deficits due to more extensive branching of the artery and less ischemic response. In contrast, the most proximal occlusions result in widespread effects that can lead to significant cerebral edema, increased intracranial pressure, loss of consciousness and could even be fatal.[1] In such occasions, mannitol (osmotic diuretic) or hypertonic saline are given to draw fluid out of the oedematus cerebrum to minimise secondary injury. Hypertonic saline is better than mannitol, as mannitol being a diuretic will decrease the mean arterial pressure and since cerebral perfusion is mean arterial pressure minus intracranial pressure, mannitol will also cause a decrease in cerebral perfusion. Contralateral hemiparesis and hemisensory loss of the face, upper and lower extremities is the most common presentation of MCA syndrome.[1] Lower extremity function is more spared than that of the faciobrachial region.[2] The majority of the primary motor and somatosensory cortices are supplied by the MCA and the cortical homunculus can, therefore, be used to localize the defects more precisely.it is important to note that middle cerebral artery lesions mostly affect the dominant hemisphere i.e. the left cerebral hemisphere.
Robot helps disabled patients regain control of their hands 1
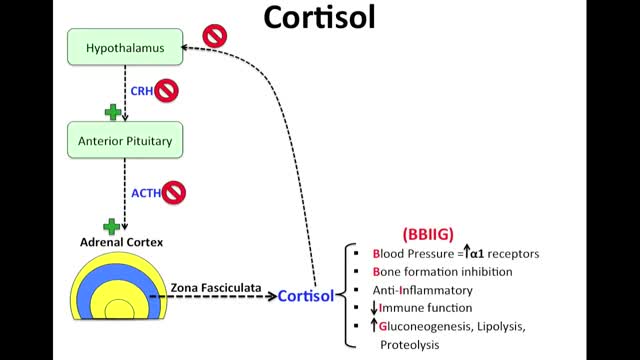
Cushing syndrome occurs when your body is exposed to high levels of the hormone cortisol for a long time. Cushing syndrome, sometimes called hypercortisolism, may be caused by the use of oral corticosteroid medication. The condition can also occur when your body makes too much cortisol on its own. Too much cortisol can produce some of the hallmark signs of Cushing syndrome — a fatty hump between your shoulders, a rounded face, and pink or purple stretch marks on your skin. Cushing syndrome can also result in high blood pressure, bone loss and, on occasion, type 2 diabetes. Treatments for Cushing syndrome can return your body's cortisol production to normal and noticeably improve your symptoms. The earlier treatment begins, the better your chances for recovery.

BACKGROUND: Clubfoot occurs in approximately one in 1000 live births and is one of the most common congenital birth defects. Although there have been several reports of successful treatment of idiopathic clubfoot with the Ponseti method, the use of this method for the treatment of other forms of clubfoot has not been reported. The purpose of the present study was to evaluate the early results of the Ponseti method when used for the treatment of clubfoot associated with distal arthrogryposis. METHODS: Twelve consecutive infants (twenty-four feet) with clubfoot deformity associated with distal arthrogryposis were managed with the Ponseti method and were retrospectively reviewed at a minimum of two years. The severity of the foot deformity was classified according to the grading system of Diméglio et al. The number of casts required to achieve correction was compared with published data for the treatment of idiopathic clubfoot. Recurrent clubfoot deformities or complications during treatment were recorded. RESULTS: Twenty-two clubfeet in eleven patients were classified as Diméglio grade IV, and two clubfeet in one patient were classified as Diméglio grade II. Initial correction was achieved in all clubfeet with a mean of 6.9 +/- 2.1 casts (95% confidence interval, 5.6 to 8.3 casts), which was significantly greater than the mean of 4.5 +/- 1.2 casts (95% confidence interval, 4.3 to 4.7 casts) needed in a cohort of 219 idiopathic clubfeet that were treated during the same time period by the senior author with use of the Ponseti method (p = 0.002). Six feet in three patients had a relapse after initial successful treatment. All relapses were related to noncompliance with prescribed brace wear. Four relapsed clubfeet in two patients were successfully treated with repeat casting and/or tenotomy; the remaining two relapsed clubfeet in one patient were treated with extensive soft-tissue-release operations.

Mitral valve surgery is surgery to either repair or replace the mitral valve in your heart. Blood flows from the lungs and enters a pumping chamber of the heart called the left atrium. The blood then flows into the final pumping chamber of the heart called the left ventricle. The mitral valve is located between these two chambers. It makes sure that the blood keeps moving forward through the heart. You may need surgery on your mitral valve if: The mitral valve is hardened (calcified). This prevents blood from moving forward through the valve. The mitral valve is too loose. Blood tends to flows backward when this occurs. Minimally invasive mitral valve surgery is done through several small cuts. Another type of operation, open mitral valve surgery requires a larger cut.

Bone marrow is the soft, sponge-like material found inside bones. It contains immature cells known as hematopoietic or blood-forming stem cells. (Hematopoietic stem cells are different from embryonic stem cells. Embryonic stem cells can develop into every type of cell in the body.) Hematopoietic stem cells divide to form more blood-forming stem cells, or they mature into one of three types of blood cells: white blood cells, which fight infection; red blood cells, which carry oxygen; and platelets, which help the blood to clot. Most hematopoietic stem cells are found in the bone marrow, but some cells, called peripheral blood stem cells (PBSCs), are found in the bloodstream. Blood in the umbilical cord also contains hematopoietic stem cells. Cells from any of these sources can be used in transplants.
Every woman is different. So are her experiences of pregnancy. Not every woman has the same symptoms or even the same symptoms from one pregnancy to the next. Also, because the early symptoms of pregnancy often mimic the symptoms you might experience right before and during menstruation, you may not realize you're pregnant. What follows is a description of some of the most common early symptoms of pregnancy. You should know that these symptoms may be caused by other things besides being pregnant. So the fact that you notice some of these symptoms does not necessarily mean you are pregnant. The only way to tell for sure is with a pregnancy test.

Anybody can and anybody should learn how to perform CPR (Cardiopulmonary resuscitation): According to the American Heart Association, a stunning 70% of Americans don’t know how what to do if somebody is experiencing a cardiac emergency because they don’t know how to administer CPR or they forgot the exact technique. This is especially alarming since almost 90% of cardiac arrests occur at home — where patients depend on the immediate respiratory care response of their family members. In brief, knowing how to perform CPR can save the life of a loved one someday.
Dark Circles around Eyes
contact lens for beginners
Sickle cell anemia is an inherited form of anemia: This is a condition in which there aren't enough healthy red blood cells to carry adequate oxygen throughout your body. Normally, your red blood cells are flexible and round, moving easily through your blood vessels. In sickle cell anemia, the red blood cells become rigid and sticky and are shaped like sickles or crescent moons. These irregularly shaped cells can get stuck in small blood vessels, which can slow or block blood flow and oxygen to parts of the body. There's no cure for most people with sickle cell anemia. However, treatments can relieve pain and help prevent further problems associated with sickle cell anemia.

Treatment may include: Rest. Ice or heat. Nonsteroidal anti-inflammatory medications. Strengthening exercises. Ultrasound therapy. Corticosteroid injection. Surgery (for severe injuries)
The occurrence and extent of cerebral infarction is determined by three basic factors: i) site of arterial occlusion, ii) the rapidity of arterial occlusion, and iii) the presence or absence of collateral circulation. Grossly, infarcts are usually divided into pale (non-hemorrhagic) and hemorrhagic types. Infarcts evolve over time, thus their gross appearance gives a clue to when they occurred. The temporal evolution of an infarct occurs in three stages: i) acute (1 day – 1 week) – the involved area is soft and edematous and there is a blurring of anatomic detail; ii) subacute (1 week – 1 month) – there is obvious tissue destruction and liquefactive necrosis of the involved brain; iii) chronic (>1 month) – the damaged tissue has been phagocytized and there is cavition with surrounding gliosis. Microscopically there is also a temporal evolution of cerebral infarcts. During the earliest phase of infarction (0-48 hours) chromatolysis and swollen eosinophilic neurons are seen. Neuronal cell necrosis and an acute inflammatory response are usually seen from 24-72 hours. This response is typically followed by an influx of mononuclear cells which begin to phagocytize necrotic debris (3-5 days). From 1-2 weeks after the infarct there is vascular proliferation and reactive astrocytosis. Over time (>1 month) the necrotic tissue will be completely removed and a cystic cavity surrounded by a glial scar will be formed.

The vertebrae are the bony building blocks of the spine. Between each of the largest parts (bodies) of the vertebrae are the discs. Ligaments are situated around the spine and discs. The spine has seven vertebrae in the neck (cervical vertebrae), 12 vertebrae in the mid-back (thoracic vertebrae), and five vertebrae in the low back (lumbar vertebrae). In addition, in the mid-buttock, beneath the fifth lumbar vertebra, is the sacrum, followed by the tailbone (coccyx).

Every 10 minutes, someone is added to the national transplant waiting list, and every day, 22 people on average die waiting for a match, according to the United Network for Organ Sharing. But, thanks to innovations in bioengineering, all of that could change. Conceived nearly 60 years ago, the total artificial heart (TAH) has helped sustain the sickest biventricular failure patients waiting for a transplant. While the design of the primary TAH used today has mostly remained stagnant since the ’80s, when it was first implanted in a patient, new models and clinical trials may lead to a better device and, one day, a permanent solution. “We are still many years away from that,” Dr. Nader Moazami, director of the Cardiac Transplantation and Ventricular Assist Device Therapy Program at the Cleveland Clinic, told FoxNews.com of a permanent artificial heart. “Although tremendous strides have been made, biocompatibility will always remain a challenge.”
The cause of schizophrenia is still unclear. Some theories about the cause of this disease include: genetics (heredity), biology (abnormalities in the brain’s chemistry or structure); and/or possible viral infections and immune disorders.
