- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Every 10 minutes, someone is added to the national transplant waiting list, and every day, 22 people on average die waiting for a match, according to the United Network for Organ Sharing. But, thanks to innovations in bioengineering, all of that could change. Conceived nearly 60 years ago, the total artificial heart (TAH) has helped sustain the sickest biventricular failure patients waiting for a transplant. While the design of the primary TAH used today has mostly remained stagnant since the ’80s, when it was first implanted in a patient, new models and clinical trials may lead to a better device and, one day, a permanent solution. “We are still many years away from that,” Dr. Nader Moazami, director of the Cardiac Transplantation and Ventricular Assist Device Therapy Program at the Cleveland Clinic, told FoxNews.com of a permanent artificial heart. “Although tremendous strides have been made, biocompatibility will always remain a challenge.”
The cause of schizophrenia is still unclear. Some theories about the cause of this disease include: genetics (heredity), biology (abnormalities in the brain’s chemistry or structure); and/or possible viral infections and immune disorders.
You may have a lot of questions about epilepsy. We will help you understand the basics, answer the most common questions, and help you find resources and other information you may need. However, information alone won’t help you manage your epilepsy and find a way to cope with the effects on your daily life. You’ll need to learn how to use the information and make it work for you.
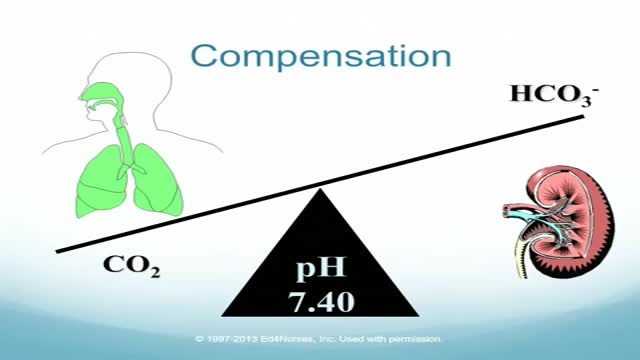
Four-Step Guide to ABG Analysis Is the pH normal, acidotic or alkalotic? Are the pCO2 or HCO3 abnormal? Which one appears to influence the pH? If both the pCO2 and HCO3 are abnormal, the one which deviates most from the norm is most likely causing an abnormal pH. Check the pO2. Is the patient hypoxic?

The Babies Hooked On Heroin |

Sex easily falls to the wayside during pregnancy. Research shows that good sex has a significant impact upon not just the relationship, but also a woman’s ability to have an easeful and even joyful birth. Unfortunately, sex during pregnancy can be quite complicated for a variety of physical and emotional reasons. This week’s video will outline how to overcome these hurdles and make sure you continue to enjoy the wonders of sex as you embark on the first steps of parenthood.
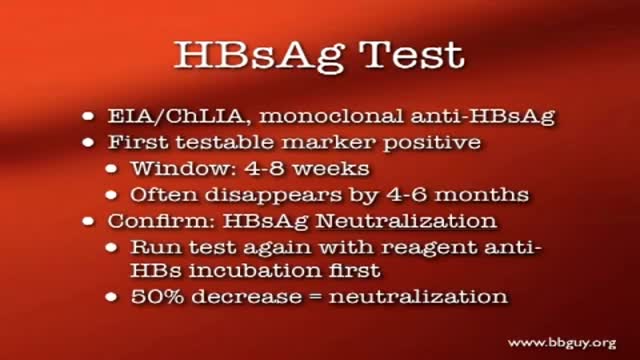
Blood Transfusion-Transmitted Diseases

If you suspect that you have sleep apnea, the usual first step is to discuss your suspicions with your primary care physician. If you don’t have a primary care physician, you can go directly to a clinician who is a sleep specialist. But check your health care insurance coverage first. Some policies require you to see a primary care physician first, and some policies limit the sleep centers and testing facilities whose services they will pay for. Unfortunately, you may discover that your policy offers limited or no coverage for the diagnosis and treatment of sleep apnea, in which case you may wish to switch insurers if and when you can.

Allergic bronchopulmonary aspergillosis (ABPA) is a condition characterised by an exaggerated response of the immune system (a hypersensitivity response) to the fungus Aspergillus (most commonly Aspergillus fumigatus). It occurs most often in patients with asthma or cystic fibrosis.
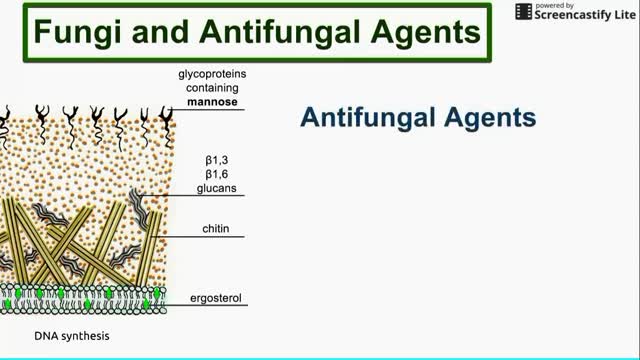
This is a brief overview of antifungal agents, their mechanisms of action, and some fungi that they affect.
Because of his weight, Jimmie Jones was on the waiting list for a new kidney for 17 years. University of Illinois Hospital surgeons used robotic surgery to give him a life without dialysis.

Inserting the Enlite Sensor with insulin pump

8 months until the world’s first human head transplant

Broca's Aphasia (expressive) When a stroke injures the frontal regions of the left hemisphere, different kinds of language problems can occur. This part of the brain is important for putting words together to form complete sentences. Injury to the left frontal area can lead to what is called Broca's aphasia.

Breastfeeding attachment Attaching your baby at the breasT
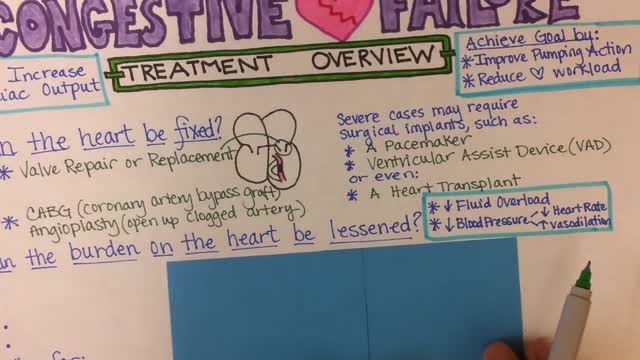
Congestive Heart Failure
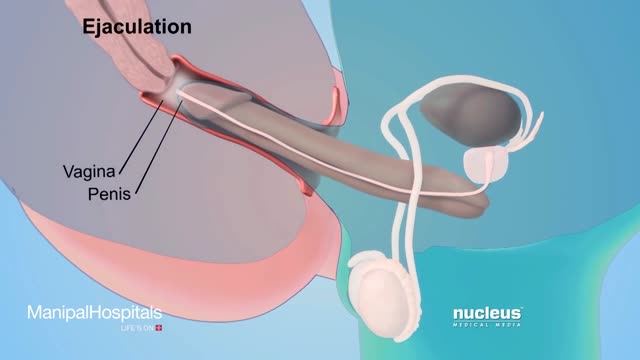
How To Use Male Condom Correctl
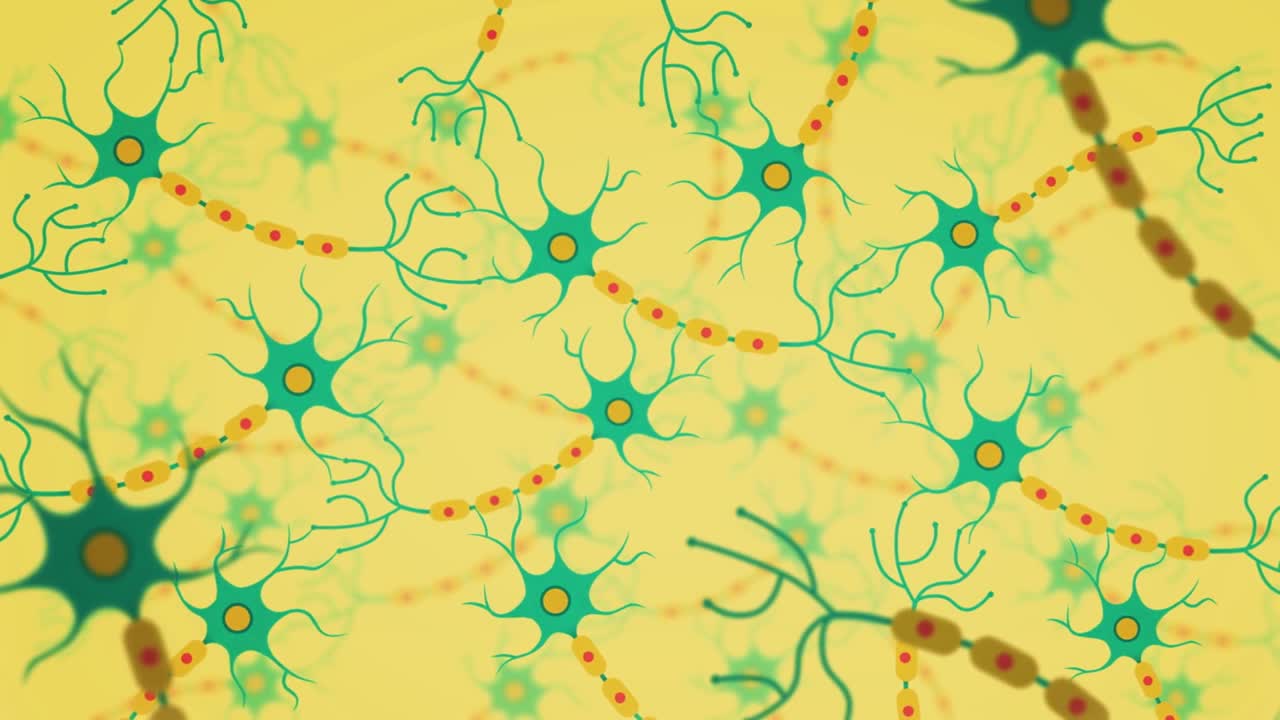
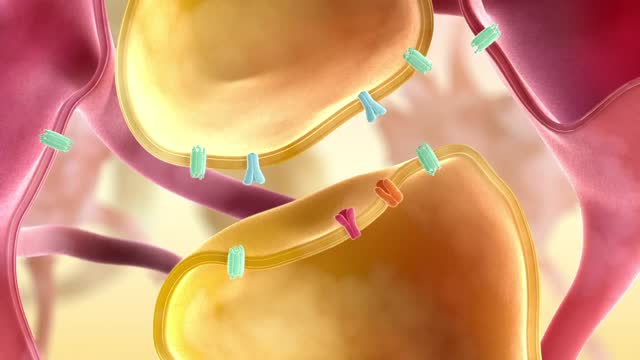
The brain is made up of billions of nerve cells that are specially designed to communicate with each other. They form many connections with one another, creating an intricate network between cells.
www.lung.org > Lung Health and Diseases > Lung Disease Lookup > Silicosis Learn About Silicosis Silicosis is a lung disease caused by breathing in tiny bits of silica, a mineral that is part of sand, rock, and mineral ores such as quartz. It mostly affects workers exposed to silica dust in occupations such mining, glass manufacturing, and foundry work. Over time, exposure to silica particles causes scarring in the lungs, which can harm your ability to breathe. Key Facts There are three types of silicosis: acute, chronic, and accelerated. It occurs in workers from mines, foundries, sandblasting, and glass manufacturing. About 2 million US workers remain potentially exposed to occupational silica. There is no cure for silicosis, but it can be prevented. What Is Silicosis? There are three types of silicosis: Acute silicosis, which causes cough, weight loss, and fatigue within a few weeks or years of exposure to inhaled silica. Chronic silicosis, which appears 10 to 30 years after exposure and can affect upper lungs and sometimes cause extensive scarring. Accelerated silicosis, which occurs within 10 years of high-level exposure. Silicosis can develop within a few weeks to even decades after exposure. When people breathe silica dust, they inhale tiny particles of the mineral silica. This silica dust can cause fluid buildup and scar tissue in the lungs that cuts down your ability to breathe. This can lead to lung scarring and cough, weight loss, and fatigue.

The ideal way to clean your teeth is no mystery; even small changes in your home dental care can lead longer-lasting teeth. Typically, by age of fifty, you will have crowns, bridges, partial prostheses, and sometimes, even a full prosthesis
