- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

#lasik #eyesurgery #BusinessInsiderIndia #lasereyesurgery
Business Insider's Michelle Yan has been nearsighted since she was 9 years old. After laser eye surgery, she has 20/20. She walks us through the pre-surgery steps, the actual surgery which the doctor referred to as a spa for eyes, as well as the recovery process.
Don't miss the suggestions and recommendations she has for all those who are planning to undergo laser eye surgery for themselves, towards the end.
-----------------------------------------------
Business Insider India features the country's business heavyweights, ranging from start-ups to veterans across industries. It offers amazing synergy between India and its foreign counterpart - developed, analyzed and presented in hallmark BI Style. It covers latest news & trends on Tech, Business, Careers, Startups and Finance.
For more such content, Visit us at: https://www.businessinsider.in/
Subscribe at: https://www.youtube.com/channe....l/UC62AhAC25Ukuscqux
BI on Facebook: https://www.facebook.com/BusinessInsiderIndia/
BI on Twitter:https://twitter.com/BiIndia
BI on Instagram: https://www.instagram.com/businessinsiderin/
BI on Tiktok: https://vm.tiktok.com/GNpHXg/
What It's Like To Get Laser Eye Surgery

A video showing arthrocentesis of the knee from Harvard medical school
Surgery video of transgastric cholecystectomy
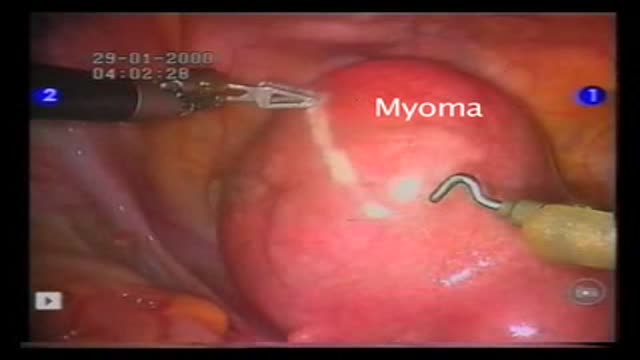
Operation performed by Dr D. Vitobello
Director of Division of Gynaecology and Obstetrics. Abano Terme Hospital, Padova (Italy)

Heart sounds S1, S2

Roux-en-Y Gastric Bypass Surgery

Coin extraction from the upper esophagus in a child.
Dr. Mohamed Abeid
From the " Endoscopy Atlas " :
http://www.facebook.com/group.php?gid=16900943915&ref=ts

A video showing Unresponsive Airway Obstruction and how to deal with it

Infant Cardio-pulmonary Resuscitation

Initial Assessment
Sentinel Lymph Node removal in breast Cancer en Français

Endoscopic third ventriculostomy in a patient with obstructive hydrocephalus

Removal of 5 Releasable sutures from the Eye
Microkeratome in Lasik

A "Hallux Valgus" or "Hallux Abducto-Valgus" deformity, is commonly referred to as a "Bunion." This describes a pathological condition involving the position of the "hallux" in relation to the first metatarsal.
A bunion deformity can clinically present with a variety of characteristics. The foot itself may present with a wide splaying of the forefoot and a painful bump on the medial aspect of the first metatarsal phalangeal joint. In addition, the hallux may be abducted from the midline of the body, with a valgus rotation in the frontal plane.
A radiographic analysis of a bunion deformity in the Anterior/Posterior or Dorsal/Plantar view will reveal a variety of pathological components. Most notably so, is the exaggerated inter-metatarsal angle between the first and second metatarsal. This may be accompanied by a displacement of the first metatarsal from its position over the sesamoids, such that the metatarsal demonstrates a medial alignment away from the sesamoids which lie to the lateral side.
In some cases, the proximal articular set angle at the head of the first metatarsal may be off-set. This "PASA" is one of the factors which determines the position of the proximal phalanx on the metatarsal during movement as well as at rest.
Although conservative care may involve shoe modifications, padding, strapping, and custom orthosis; surgical reconstruction may be required to alleviate painful and immobilizing bunion conditions.
Soft tissue components of the bunion deformity are primarily addressed by means of a capsular modification, as well as a tenotomy of the adductor tendon at its insertion on the base of the proximal phalanx. The fibular sesamoid may be repositioned by a release of the surrounding ligaments.
Surgical management of the bone or osseous components of a bunion deformity will commonly include an osteotomy and correction to re-establish a more functional position of the first metatarsal within the forefoot. This capital fragment of bone is held in place with hardware fixation in order to secure a proper alignment during the healing phase, thus allowing the hallux to return to a more functionally useful position in the sagittal plane.
A video show phlebotomy tips

Hawkin's Test

En este video, Ana Rivera, Asesor de Salud Publica para los CDC, describe la influenza o gripe porcina: sus signos y síntomas, cómo se transmite, los medicamentos para su tratamiento, las medidas que las personas pueden tomar para protegerse de esta enfermedad y lo que deben hacer las personas si se enferman

A video of Laparoscopic Cholecystectomy with Cholangiography in a Female Patient

The video will describe silhouette sign on a chest x-ray. Please see disclaimer on my website. www.academyofprofessionals.com
