- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
How To Help Your Child Learn To Read, Help My Child Learn To Read, Best Way To Teach Reading---- http://children-learning-reading.good-info.co -- how to help your child learn to read - Help My Child Learn to Read The ability to read is vital for success. It helps your child succeed in school, helps them build self-confidence, and helps to motivate your child. Being able to read will help your child learn more about the world, understand directions on signs and posters, allow them to find reading as an entertainment, and help them gather information. Learning to read is very different from learning to speak, and it does not happen all at once. There is a steady progression in the development of reading ability over time. The best time for children to start learning to read is at a very young age - even before they enter pre-school. Once a child is able to speak, they can begin developing basic reading skills. Very young children have a natural curiosity to learn about everything, and they are naturally intrigued by the printed texts they see, and are eager to learn about the sounds made by those letters. You will likely notice that your young child likes to look at books and thoroughly enjoys being read to. They will even pretend to behave like a reader by holding books and pretend to read them. As parents, you're the most important first step in your children's journey into the wonderful world of reading. It is up to you to create the most supportive environment that turns your child on to reading - such as reading aloud to them often during the day and before bedtime, and placing age appropriate books for children around the house, so that the child will have access to plenty of books. Reading often to your child will help develop their interest in books and stories, and soon they will want to read stories on their own. >>Teach your child to read and enable your child to become a fast and fluent reader! Click here to help your child learn to read http://children-learning-reading.good-info.co
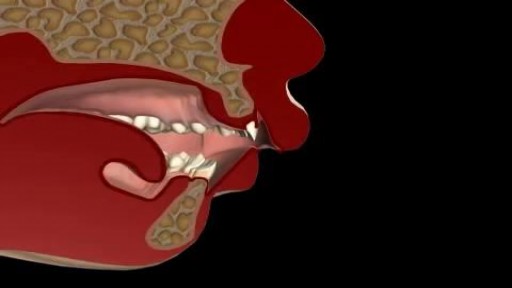
Oral and maxillofacial surgery specializes in treating many diseases, injuries and defects in the head, neck, face, jaws and the hard and soft tissues of the oral and maxillofacial region. It is an internationally recognized surgical specialty

Case of ITP with persistent very low platelet count despite best medical management

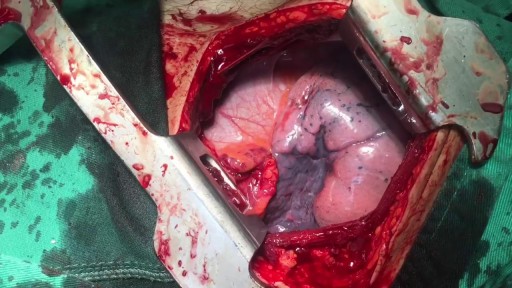
Removal of drain tube after spleen surgery


Mr Andrew Clarke, a leading surgeon and expert in laparoscopic techniques, explains how laparoscopic surgery allows a much quicker and less painful recovery than with open surgery.
Make an appointment with Mr Andrew Clarke here: https://www.topdoctors.co.uk/doctor/andrew-clarke
✔ Follow us on Instagram: https://bit.ly/3fSrqXb
✔ Follow us on Facebook: https://bit.ly/3t5kGsW
✔ Follow us on Twitter: https://bit.ly/39TidKh
Mitral valve repair

Measurement of pulse and respiratory rate

the technique of insertion of a tube into the abdomen to diagnose intra-abdominal bleeding

Thyroid status assessment and thyroid gland examination
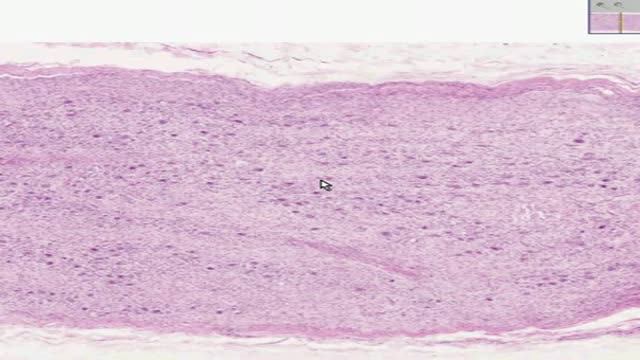
Histology of Sympathetic Ganglion

Infant Cardio-pulmonary Resuscitation
Loyola oral Presentation for Rounds video
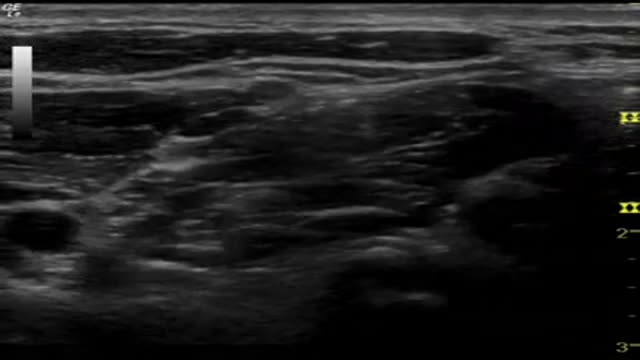
Interscalene Block
Laparoscopic Sleeve Gastrectomy Operation

Removal of 5 Releasable sutures from the Eye

Spinal Fusion operation

Spinal disc prolapse and replacement
