- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Zip Surgical Skin Closure
Factitious disorder is the term used to describe a pattern of behavior centered on the exaggeration or outright falsifications of one’s own health problems or health problems of others. Some people with this disorder fake or exaggerate physical problems; others fake or exaggerate psychological problems or a combination of physical and psychological problems. Factitious disorder differs from a pattern of falsified or exaggerated behavior called malingering. While malingerers make their claims out of a motivation for personal gain, people with factitious disorder have no such motivation.
Good and Bad Foods to Eat

Encephalitis (en-sef-uh-LIE-tis) is inflammation of the brain. Viral infections are the most common cause of the condition. Encephalitis can cause flu-like symptoms, such as a fever or severe headache. It can also cause confused thinking, seizures, or problems with senses or movement. However, many cases of encephalitis result in only mild flu-like symptoms or even no symptoms. Severe cases of encephalitis, while relatively rare, can be life-threatening. Because the course of any single case of encephalitis can be unpredictable, it's important to get a timely diagnosis and treatment.

Pancreatitis is inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum—the first part of the small intestine. The pancreas secretes digestive juices, or enzymes, into the duodenum through a tube called the pancreatic duct. Pancreatic enzymes join with bile—a liquid produced in the liver and stored in the gallbladder—to digest food. The pancreas also releases the hormones insulin and glucagon into the bloodstream. These hormones help the body regulate the glucose it takes from food for energy. Normally, digestive enzymes secreted by the pancreas do not become active until they reach the small intestine. But when the pancreas is inflamed, the enzymes inside it attack and damage the tissues that produce them. Pancreatitis can be acute or chronic. Either form is serious and can lead to complications. In severe cases, bleeding, infection, and permanent tissue damage may occur.

Fake Sonogram
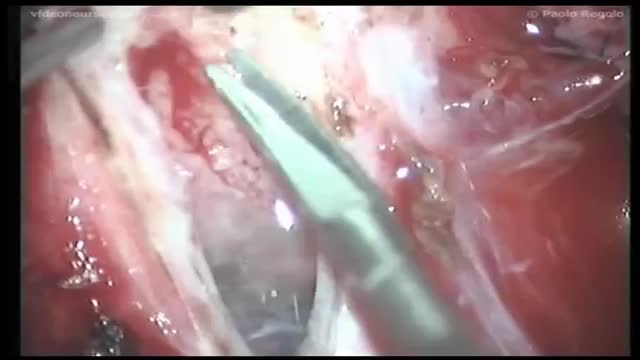
The annual incidence of primary intraspinal neoplasm is approximately five per million for females and three per million for males.[9] Spinal intradural extramedullary tumors account for two thirds of all intraspinal neoplasms and include neuromas and meningiomas.[1] Overall, meningiomas account for 25 to 46% of primary spinal neoplasms and are the second most common intradural spine tumor after neuromas.[9] Spinal meningiomas occur less frequently than intracranial ones and account for approximately 7.5 to 12.7% of all meningiomas.[25]
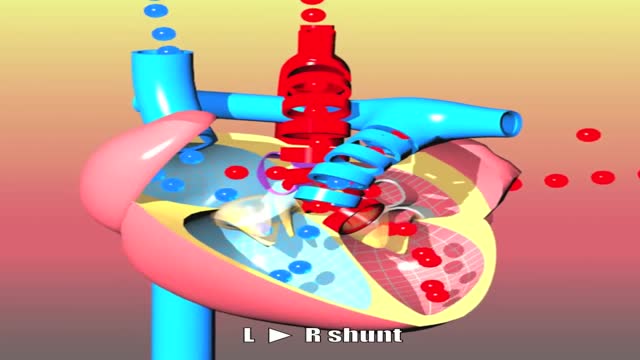
Congenital heart defects I: ASD, VSD, AS, PS, PDA and PFO
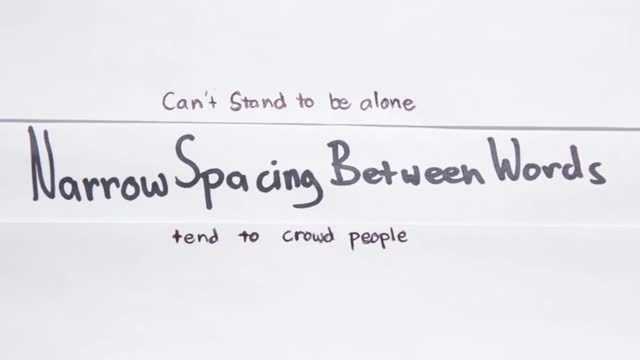
What Your Handwriting Says About You
What is your mental age?
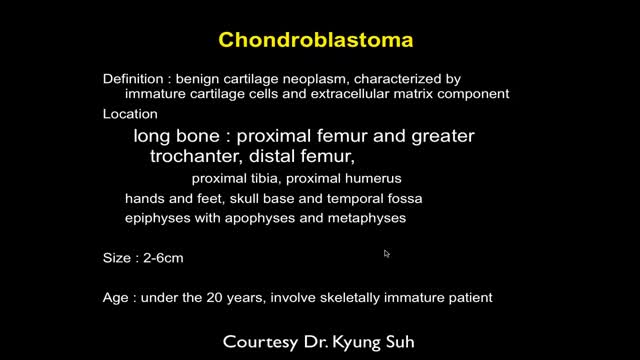
MRI of Bone Tumor
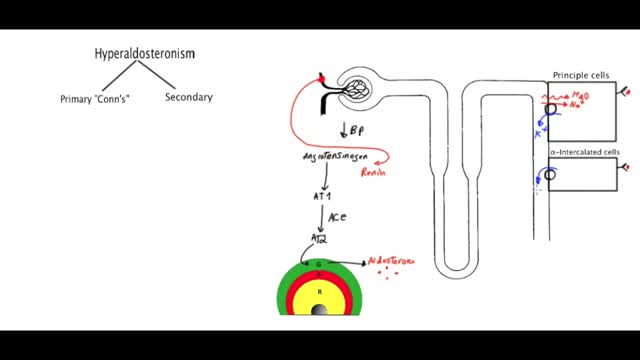
Primary aldosteronism, also known as primary hyperaldosteronism or Conn's syndrome, is excess production of the hormone aldosterone by the adrenal glands resulting in low renin levels. Often it produces few symptoms. Most people have high blood pressure which may cause poor vision or headaches.

See the effects of cannabis first hand, unedited, on Parkinson's tremor dyskinesia, and voice.
Bengmark Naso-Intestinal tube

What causes addiction? Easy, right? Drugs cause addiction. But maybe it is not that simple.

Tongue-tie (ankyloglossia) is a condition present at birth that restricts the tongue's range of motion. With tongue-tie, an unusually short, thick or tight band of tissue (lingual frenulum) tethers the bottom of the tongue's tip to the floor of the mouth

Tenosynovitis is inflammation of the lining of the sheath that surrounds a tendon (the cord that joins muscle to bone).

Everyone feels sad or low sometimes, but these feelings usually pass with a little time. Depression—also called “clinical depression” or a “depressive disorder”—is a mood disorder that causes distressing symptoms that affect how you feel, think, and handle daily activities, such as sleeping, eating, or working. To be diagnosed with depression, symptoms must be present most of the day, nearly every day for at least 2 weeks.

Simple interrupted suturing is the most basic and most important of the suturing techniques.
LICHTENSTEIN TENSION FREE HERNIOPLASTY FOR INDIRECT INGUINAL HERNIA
