- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Resection of transverse colostomy prolapse

Busadagur í fss 2008

Fibroma Excision in the Cheek
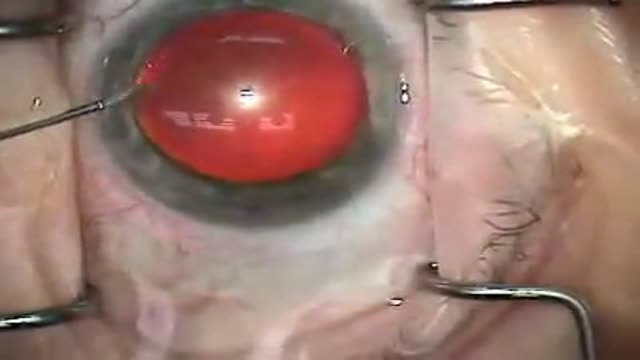
A video of modern cataract surgery employing a temporal, clear-corneal approach with topical anesthesia and ultrasound phacoemulsification; an aspheric silicone lens implant is inserted
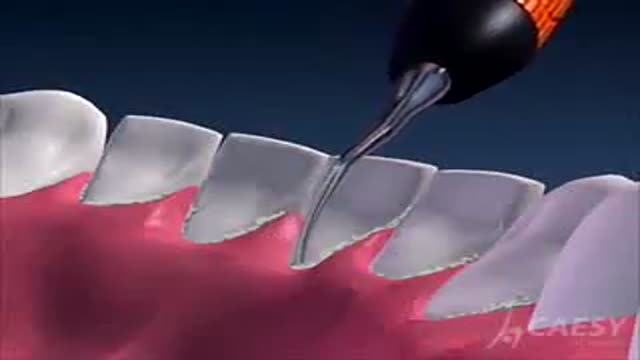
Ultrasonic Scaling

Cataract surgery with dense arcus

New Techniques for Dental Crowns and Bridges

Using a common laser for treatment of eye cancer may benefit some patients by preserving site.

nurses removing chest tube from surgery after spontaneous pneumothorax

Fractured implant extraction
A patient suffering from Trigeminal Neuralgia (extreme facial pain) has breakthrough neurosurgery, microvascular decompression, to resolve the pain & restore quality of life.~ Detroit Medical Center

Losing Weight- Gaining Health with LapBand Surgery video

A DMC patient suffering from an abdominal aortic aneurysm receives an endovascular graft to alleviate the potentially deadly problem, performed by DMC cardiac specialist Dr. Ali Kafi. ~ Detroit Medical Center
The video will describe what is the purpose of a very important blood test known as ABGs. Please see my website for disclaimer.
The video will discuss a few things that are used to treat pulmonary embolism. Please see my website for disclaimer.
Learn ECG in a dance..lol
The video will describe how cavitating lesions appear on a chest x-ray. Please see my website for disclaimer.
The video will describe difference between oxidation and oxygenation. Please see my website for disclaimer.

The video will describe position of several tubes and lines that may be visible on a chest x-ray. Please see my website for discliamer.

This is a video showing how to secure a venipuncture
