- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
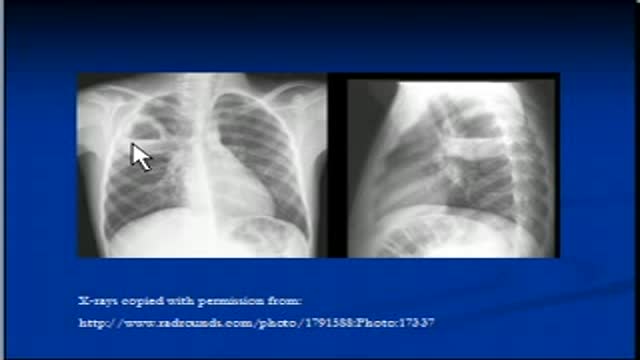
The video will describe how cavitating lesions appear on a chest x-ray. Please see my website for disclaimer.
The video will describe difference between oxidation and oxygenation. Please see my website for disclaimer.

The video will describe position of several tubes and lines that may be visible on a chest x-ray. Please see my website for discliamer.

This is a video showing how to secure a venipuncture

The video will describe what is miliary tuberculosis. Please see my website for disclaimer.

Endotracheal Intubation During General Anaesthesia

تكبير الثدي تكبير الصدر تجميل الثدي تجميل الصدر

Secondary Cataract
Dr. Samir Abd Elghaffar, Associate professor of Intervntional Radiology at Ain Shams University, Faculty of Medicine is illustrating a live Microwave Ablation of Hepatic Focal Lesion discussing the differences between Radio Frequency ablation RFA and Microwave Ablation.

Chapel Hill Tubal Reversal Center - www.tubal-reversal.net - illustrates proper hand hygiene technique for surgical scrub to disinfect the hands prior to entering the operating room for tubal ligation reversal surgery.

Medically: Pain with Intercourse; the medical reason and dealing with pain during intercourse.
Prostate Health and Cancer Seminar features nationally renowned physicians and scientists presenting the most current study and practices for the diagnosis and treatment of prostate cancer. This day-long program offers in-depth exploration of prostate issues that range from monitoring PSA counts to cutting-edge research to current treatment trends.

Undiagnosed severe condition. 26th week of pregnancy. Sorry, I am reviewing the images, it is not a holoprosencephaly; more likely: corpus callosum agenesis. Please feedback

AL EMADI HOSPITAL-QATAR-DOHA

Nissen Laparoscopic Fundoplication Acid Reflux Surgery Stomach
Ovulation
Closed Cuff Surgical Gloving
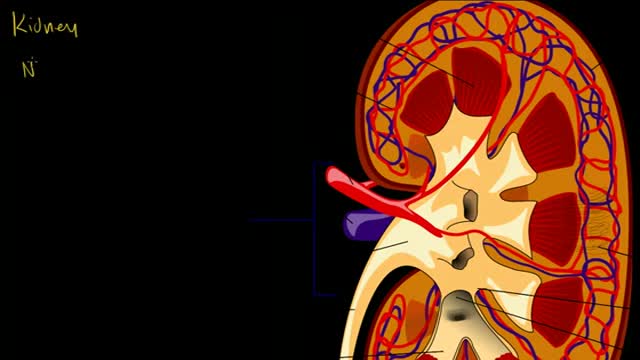
Kidney and Nephron

Diabetes Insipidus Symptoms

From fabric choices to layering, clothing tips to help you deal with menopausal hot flashes
