- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Body-Safe Sex Toys
SEX WITH DIAPHRAGM TO CONTROL UNWANTED PREGNANCY
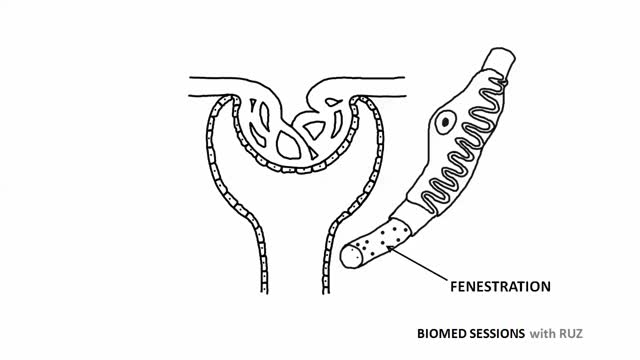
Glomerular filtration is the first step in making urine. It is the process that your kidneys use to filter excess fluid and waste products out of the blood into the urine collecting tubules of the kidney, so they may be eliminated from your body.

Inside the living body

This minimally invasive surgical procedure repairs the valve without removing the old, damaged valve. Instead, it wedges a replacement valve into the aortic valve’s place. The surgery may be called a transcatheter aortic valve replacement (TAVR) or transcatheter aortic valve implantation (TAVI).

Blood type (or blood group) is determined, in part, by the ABO blood group antigens present on red blood cells. A blood type (also called a blood group) is a classification of blood based on the presence or absence of inherited antigenic substances on the surface of red blood cells (RBCs).

wound clean from pus

Surfactant. Surfactants are compounds that lower the surface tension (or interfacial tension) between two liquids or between a liquid and a solid. Surfactants may act as detergents, wetting agents, emulsifiers, foaming agents, and dispersants.

1500 mg of sodium amounts to 0.75 teaspoons or 3.75 grams of salt per day, while 2300 mg amounts to one teaspoon or 6 grams of salt per day. Most people today are eating much more than that. The average intake of sodium is about 3400 mg, most of it coming from processed foods.
Large Facial Tumor Removal, Parotid Gland
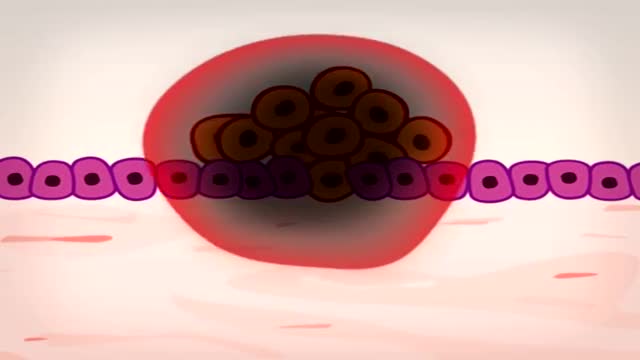
In 5 minutes find out how and why a normal cell becomes a cancer cell: risk factors and treatment.
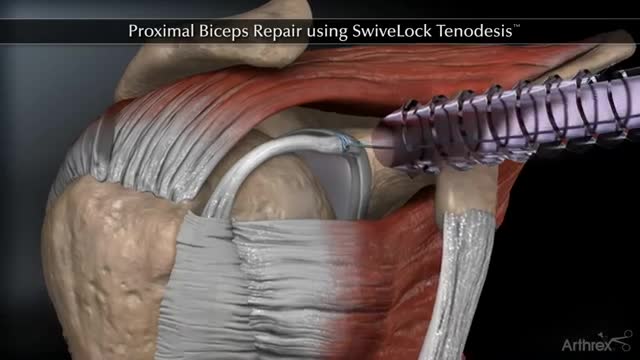
Proximal Biceps Repair using SwiveLock Tenodesis

Three lower limb surgeries that you need to know about.

your DNA Journey
Scientists reveal how LSD alters your mind.
Some common signs of spinal tumors may include the following: Pain (back and/or neck pain, arm and/or leg pain) Muscle weakness or numbness in the arms or legs. Difficulty walking. General loss of sensation. Difficulty with urination (incontinence) Change in bowel habits (retention) Paralysis to varying degrees.
3 effective home remedies to lift your “BREAST” in a natural way

Watching A Dentist Fix Tooth Decay Is Beyond Satisfying.

This is the future of medicine

This video was taken 2 weeks after this lovely patient had a Endoscopic Brow Lift, Face and Neck lift, and Fat Grafting. Know more about Handal Plastic Surgery Call us at (561) 912-9888 for more info!
