- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

How to Know If You Have a Serious Knee Injury or Problem
Youtube Channel: https://www.youtube.com/user/physicaltherapyvideo
Website: https://bobandbrad.com/
Bob & Brad discuss how to know if you have a serious knee injury. They show you what to look for and what you should do.
This Week's Giveaway:
This month we are giving away a grand prize of a Sleepovation mattress and two pillows!
BONUS: 2 runners-up will receive a Sleepovation pillow!
December Giveaway link: https://shrsl.com/2ob0e
Purchase Mattress: http://shrsl.com/1n2e2
Purchase Pillow: http://shrsl.com/1xch4
Discount: Make sure to use the discount code FAMOUSPT to receive 15% off of your purchase of a mattress or use FAMOUSPTPIL for 25% off of their pillows! This is the biggest discount of the year!
Sleepovation will reimburse winners of the giveaway if they have already purchased, so no need to wait to buy Bob & Brad's favorite mattress and pillow!
Our videos offer the best "get fit , stay healthy, and pain-free" information directed toward people 0 to 101 years old. Physical Therapists Bob Schrupp and Brad Heineck have over 50 years of combined. We try to add a twist of our humor into each video in our quest to be the "Most Famous Physical Therapists on the Internet" In our opinion of course!!! Subscribe to us now and join the fun. Not only will these videos provide outstanding health information on treating yourself at home, we also do product reviews.
For our favorite products on Amazon click on this link: https://www.amazon.com/shop/physicaltherapyvideo
Visit us on our other social media platforms:
Website: https://bobandbrad.com/
Facebook: https://www.facebook.com/BobandBrad/
Instagram: https://www.instagram.com/officialbobandbrad/
Twitter: https://twitter.com/ptfamous
Bob and Brad’s Products:
Grip and Forearm Strengthener: https://store.bobandbrad.com
Wall Anchor: https://store.bobandbrad.com
Booyah Stik: https://store.bobandbrad.com
Knee Glide: https://store.bobandbrad.com
Fit Glide: https://store.bobandbrad.com
Massage Gun: https://amzn.to/36pMekg
Hanging Handles: https://amzn.to/2RXLVFF
Resistance Bands: https://amzn.to/36uqnbr
Pull Up Bands: https://amzn.to/3qmI4Rv
If you order from the Bob and Brad Store Links, you will receive 15% off your purchase.
Check out our shirts, mugs, bags and more in our Bob and Brad merchandise shop here: https://shop.spreadshirt.com/bob-brad
Bob & Brad Amazon Store: https://amzn.to/2RTSLLh
Other Products We Love: https://www.amazon.com/shop/physicaltherapyvideo?listId=3581Z1XUVFAFY
Check out The Bob & Brad Crew on YouTube by clicking here: https://www.youtube.com/c/thebobbradcrew
Want to help translate our videos? We would so love the help! http://www.youtube.com/timedtext_cs_panel?c=UCmTe0LsfEbpkDpgrxKAWbRA&tab=2
Medical Disclaimer All information, content, and material of this website is for informational purposes only and are not intended to serve as a substitute for the consultation, diagnosis, and/or medical treatment of a qualified physician or healthcare provider.
Affiliate disclaimer: Keep in mind that we may receive commissions when you click our links and make purchases. However, this does not impact our reviews and comparisons. We are highly selective in our products and try our best to keep things fair and balanced in order to help you make the best choice for you.

Traditionally, the appendix is removed through an incision in the right lower abdominal wall. In most laparoscopic appendectomies, surgeons operate through 3 small incisions (each ¼ to ½ inch) while watching an enlarged image of the patient's internal organs on a television monitor

Cataract eye surgery

operation on the stomach

Demonstrative video of Advanced PRK - No Touch Technique. 100% Laser. In this particular technique there is no need for mechanical device or to cut the corneal flap.

Shoulder Exam
I think that the most daunting aspect of the shoulder exam is appreciating the functional anatomy of this incredibly mobile joint. The primary benefit of the ball and socket arrangement is that it allows the hand to be positioned precisely in space, maximizing our ability to function. In terms of functionality, the shoulder might be best described as having a golf ball-on-a-tee design.
Location Of The Muscle Groups Is Approximated In The Pictures Above.
Start by looking at the normal (or more normal) side. Note any scars, obvious asymmetry, discoloration, swelling, or muscle asymmetry.
Palpation
Gently palpate around the shoulder, touching each of the landmarks noted above. Make note of pain.

Laparoscopic fixation of intraabdominal testis into the scrotum in a case of undescended testis.
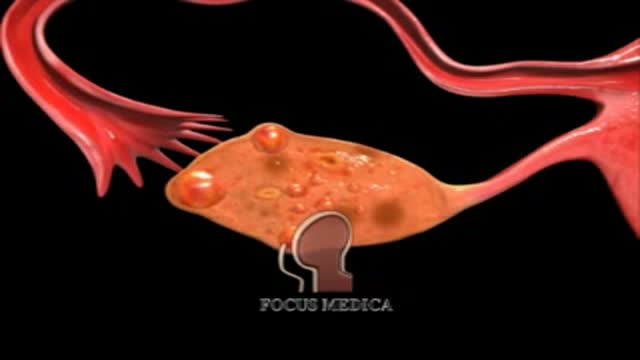
An animation showing what PCO is
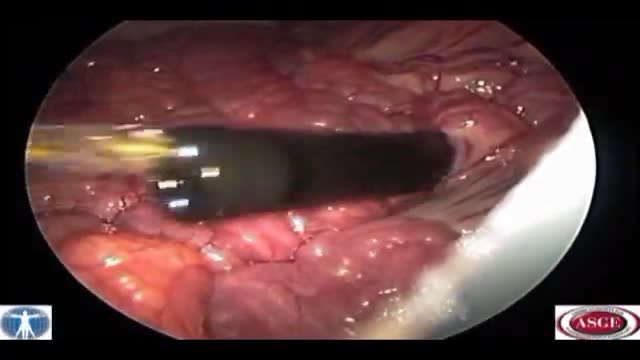
Natural Orifice Endoscopic Transgastric Distal Pancreatectomy, A Prospective Randomized Controlled Trial. Natural orifice surgery may represent a paradigm shift in the area of minimally invasive surgery and therapeutic endoscopy. However, studies to date have been limited primarily to small ca...se series with small sample sizes. There has been no large rigorous randomized controlled trial of natural orifice surgery to date. Early work on procedures such as peritoneoscopy, oophorectomy and tubal ligation, while pioneering, have reproduced laparoscopic procedures with minimal morbidity and mortality. In contrast, distal pancreatectomy has a post-operative morbidity of more than 50% even in high volume tertiary care centers. As a highly morbid surgery, the post-operative event rate would allow for a significant difference to be seen in a trial of conventional versus NOTES distal pancreatectomy. We have recently completed a prospective randomized controlled trial of NOTES versus laparoscopic distal pancreatectomy in a swine model which builds on our earlier non-survival work. This video focuses on the endoscopic technique.

First aid for a choking conscious adult

Oral Surgery and Dental Implants

Combined Spinal-Epidural Obstetric Anesthesia

Laparoscopic Removal of Ovarian Cyst

Laser Liposuction for Weight Loss

Some tips on obtaining venous blood samples.

living with chronic fatigue syndrome

Securing A Chest Tube

YOU CAN READ MY MIGRAINE THEORY AND HOW TO DO AND USE MY MIGRAINE DEVICES.

Open Distal Pancreatectomy Surgery Video
The video will describe aspergilloma. Please see my website for disclaimer. www.academyofprofessionals.com
