- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Cataract Surgery Medical Eye Video
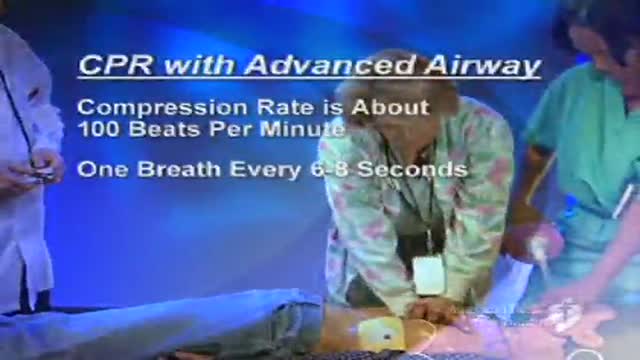
CPR in a patient with Advanced Airway Managment such as a patient with endotracheal tube or combitube is different than performin normal CPR. This video shows how to perform that.
Jane Seymour sheds light on atrial fibrillation and AF-related stokes.
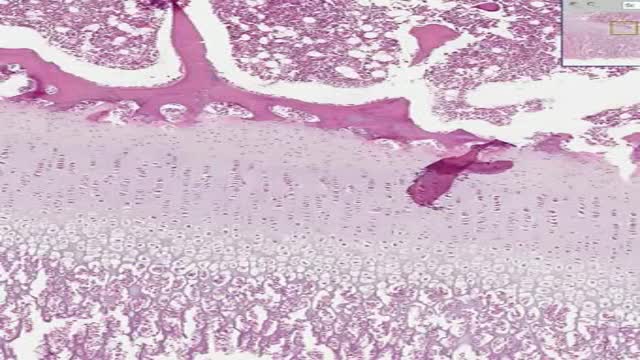
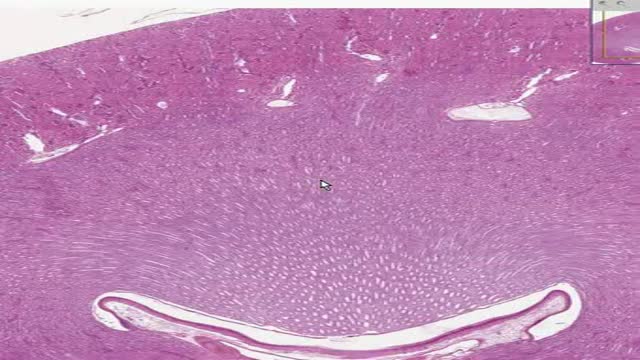
Histology of Endochondral Ossification
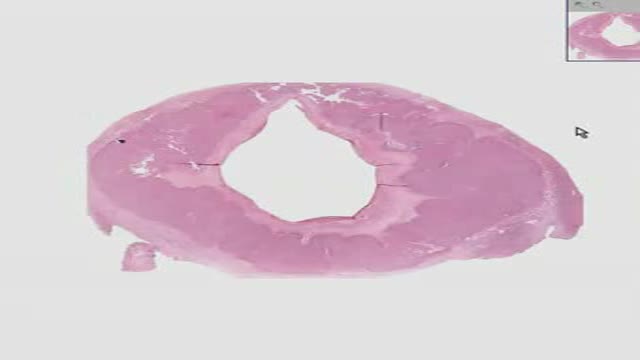
Histology of Kidney
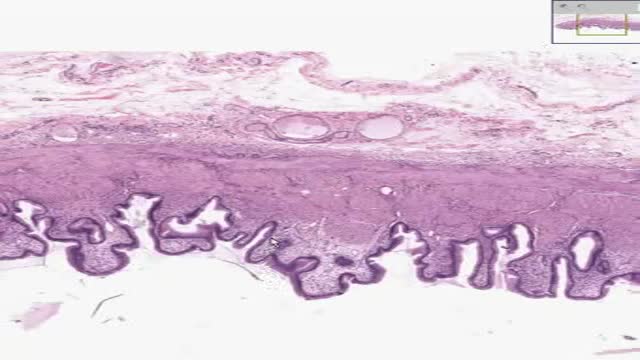
Histology of Gall Bladder

Histology of Adrenal
Histology of Corpus Luteum 1
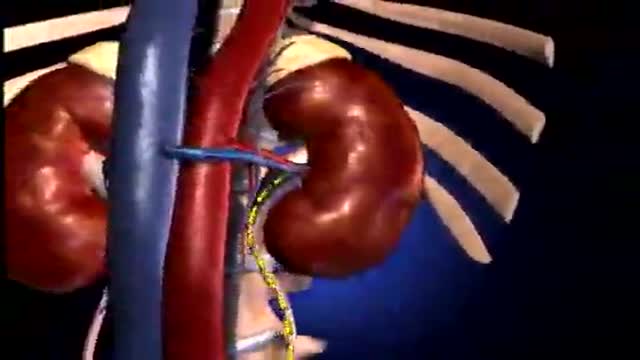
The Nephron Functional Unit of Kidney

Mechanism of Type 2 Diabetes Animation

Traumatic Urinary Bladder Groin Injury
ADA IS ABSOLUTE CLUELESS AND IGNORANT CONCERNING MOST INNOVATIVE DENTAL IMPLANT METHOD
http://breatheasthmafree.blog300.com - Asthma Treatments bronchitis - Bronchitis Asthma Home Remedies
Kill Asthma Today!
Natural - Treatment for Asthma
Cure & Revitalise Your Breathing
http://breatheasthmafree.blog300.com
Asthma Treatments bronchitis - Bronchitis Asthma Home Remedies
Crohns Disease Patient Education
Diverticulitis Attack Surgery
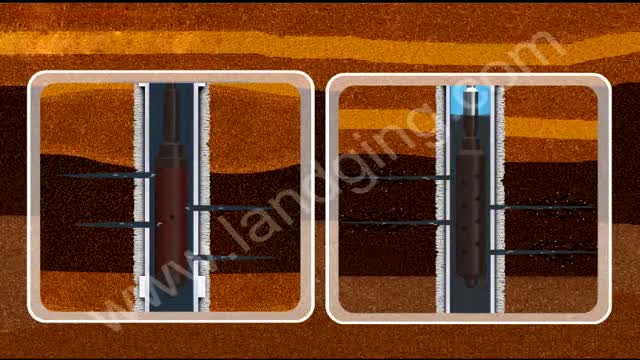
http://www.landging.com/well-test-animation.html
This well test animation demonstrates new oil drilling technology.

Holoprosencephaly (HPE, once known as arhinencephaly) is a cephalic disorder in which the prosencephalon (the forebrain of the embryo) fails to develop into two hemispheres. Normally, the forebrain is formed and the face begins to develop in the fifth and sixth weeks of human pregnancy. The condition also occurs in other species, as with Cy, the Cyclops kitten.

This video is a simplified tutorial to teach how to read and understand chaest x-rays. It is for beginners

Hair Transplant Clinic Dubai leads the way in providing amazing natural Hair Transplants results. It is Best Hair Transplant In Dubai to get your problems.
Animation about Swine Flue: Facts, Symptoms, Prevention
