- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

This video demonstrates Laparoscopic Cholecystectomy Fully Explained Skin-to-Skin Video with Near Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. A laparoscopic cholecystectomy is a minimally invasive surgical procedure that involves removing the gallbladder. It is typically performed using small incisions in the abdomen, through which a laparoscope (a thin tube with a camera and light) and surgical instruments are inserted. The surgeon uses the laparoscope to visualize the inside of the abdomen and to guide the instruments in removing the gallbladder.
Near-infrared cholangiography is a technique that uses a special camera and fluorescent dye to visualize the bile ducts during surgery. The dye is injected into the cystic duct (the tube that connects the gallbladder to the bile ducts) and the camera detects the fluorescence emitted by the dye, allowing the surgeon to see the bile ducts more clearly.
The combination of laparoscopic cholecystectomy and near-infrared cholangiography has become a standard of care in many hospitals and surgical centers. It allows for a more precise and efficient surgery, reducing the risk of complications such as bile duct injury.
The use of indocyanine green (ICG) with near-infrared imaging during laparoscopic cholecystectomy has several advantages. Here are some of them:
Better visualization of the biliary anatomy: ICG with near-infrared imaging allows for better visualization of the biliary anatomy during surgery. This helps the surgeon identify important structures, such as the cystic duct and the common bile duct, and avoid injuring them.
Reduced risk of bile duct injury: With better visualization of the biliary anatomy, the risk of bile duct injury during surgery is reduced. Bile duct injury is a serious complication that can occur during laparoscopic cholecystectomy and can lead to long-term health problems.
Improved surgical precision: ICG with near-infrared imaging also improves surgical precision. The surgeon can better see the tissues and structures being operated on, which can help reduce the risk of bleeding and other complications.
Shorter operating time: The use of ICG with near-infrared imaging can shorten the operating time for laparoscopic cholecystectomy. This is because the surgeon can more quickly and accurately identify the biliary anatomy, which can help streamline the surgery.
Overall, the use of ICG with near-infrared imaging is a valuable tool in laparoscopic cholecystectomy that can improve surgical outcomes and reduce the risk of complications.
Like any surgical procedure, laparoscopic cholecystectomy (gallbladder removal) has potential complications. Here are some of the most common ones:
Bleeding: Bleeding during or after the surgery is a possible complication of laparoscopic cholecystectomy. Most cases are minor and can be easily controlled, but in rare cases, significant bleeding may require a blood transfusion or even additional surgery.
Infection: Any surgical procedure carries a risk of infection. After laparoscopic cholecystectomy, there is a risk of infection at the site of the incisions or within the abdomen. Symptoms may include fever, pain, redness, or drainage from the incision sites.
Bile leakage: In some cases, a small amount of bile may leak from the bile ducts into the abdominal cavity after gallbladder removal. This can cause abdominal pain, fever, and sometimes requires further surgery or treatment.
Injury to nearby organs: During the surgery, there is a small risk of unintentional injury to nearby organs such as the liver, intestines, or bile ducts. This can cause additional complications and may require further treatment.
Adverse reactions to anesthesia: As with any surgery requiring general anesthesia, there is a small risk of adverse reactions to the anesthesia, such as an allergic reaction, respiratory problems, or heart complications.
Most patients recover without complications following a laparoscopic cholecystectomy, but it is important to discuss any concerns or questions with your surgeon beforehand.
Contact us
World Laparoscopy Hospital
Cyber City, Gurugram, NCR Delhi
INDIA : +919811416838
World Laparoscopy Training Institute
Bld.No: 27, DHCC, Dubai
UAE : +971525857874
World Laparoscopy Training Institute
8320 Inv Dr, Tallahassee, Florida
USA : +1 321 250 7653
Regenerate response

hemisplenectomy is removal of the half of the spleen.It was done firstly in Azerbaijan by prof. Dr Med Qurban Muslimov in 12 years old child with simple syst of the spleen.

The period between stages one and two of labour
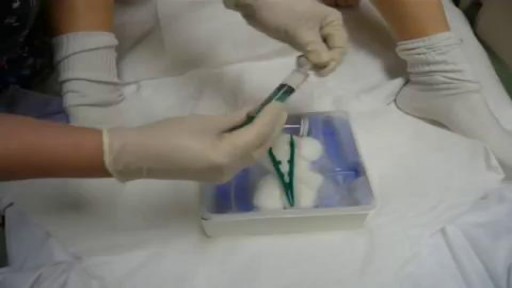
Watch that Female Foley Catheter Insertion Procedure
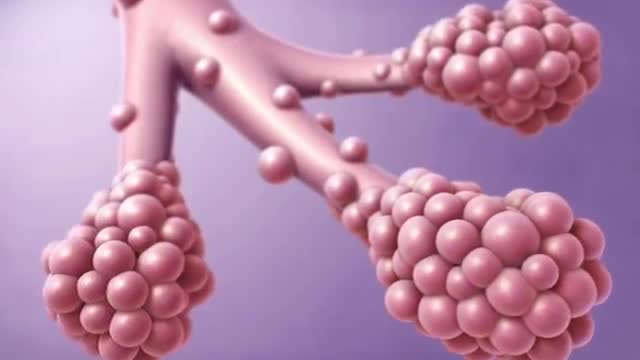
Idiopathic pulmonary fibrosis (IPF) is defined as a specific form of chronic, progressive fibrosing interstitial pneumonia of unknown cause, primarily occurring in older adults, limited to the lungs, and associated with the histopathologic and/or radiologic pattern of usual interstitial pneumonia (UIP).[1] Signs and symptoms The clinical symptoms of idiopathic pulmonary fibrosis are nonspecific and can be shared with many pulmonary and cardiac diseases. Most patients present with a gradual onset (often >6 mo) of exertional dyspnea and/or a nonproductive cough. Approximately 5% of patients have no presenting symptoms when idiopathic pulmonary fibrosis is serendipitously diagnosed.
Vaginal discharge serves an important housekeeping function in the female reproductive system. Fluid made by glands inside the vagina and cervix carries away dead cells and bacteria. This keeps the vagina clean and helps prevent infection. Most of the time, vaginal discharge is perfectly normal. The amount can vary, as can odor and hue (its color can range from clear to a milky white-ish), depending on the time in your menstrual cycle. For example, there will be more discharge if you are ovulating, breastfeeding, or are sexually aroused. The smell may be different if you are pregnant or you haven't been diligent about your personal hygiene. None of those changes is cause for alarm. However, if the color, smell, or consistency seems significantly unusual, especially if it accompanied by vaginal itching or burning, you could be noticing an infection or other condition. What causes abnormal discharge? Any change in the vagina's balance of normal bacteria can affect the smell, color, or discharge texture. These are a few of the things that can upset that balance:

What factors should I consider when deciding whether to have surgery? The following factors should be considered when deciding whether to have surgery: Your age—If you have surgery at a young age, there is a chance that prolapse will recur and may possibly require additional treatment. If you have surgery at an older age, general health issues and any prior surgery may affect the type of surgery that you have. Your childbearing plans—Ideally, women who plan to have children (or more children) should postpone surgery until their families are complete to avoid the risk of prolapse happening again after corrective surgery. Health conditions—Any surgical procedure carries some risk, such as infection, bleeding, blood clots in the legs, and problems related to anesthesia. Surgery may carry more risks if you have a medical condition, such as diabetes, heart disease, or breathing problems, or if you smoke or are obese. New problems—Surgery also may cause new problems, such as pain during sex, pelvic pain, or urinary incontinence.

Frostbite is an injury caused by freezing of the skin and underlying tissues. First your skin becomes very cold and red, then numb, hard and pale. Frostbite is most common on the fingers, toes, nose, ears, cheeks and chin. Exposed skin in cold, windy weather is most vulnerable to frostbite. But frostbite can occur on skin covered by gloves or other clothing. Frostnip, the first stage of frostbite, doesn't cause permanent skin damage. You can treat very mild frostbite with first-aid measures, including rewarming your skin. All other frostbite requires medical attention because it can damage skin, tissues, muscle and bones. Possible complications of severe frostbite include infection and nerve damage.

Haemorrhoids is one of the most common problems seen in surgical OPD. Open haemorrhoidectomy has remained the gold standard for a long time with a high post-operative morbidity. The quest for a better understanding of the pathology of haemorrhoids resulted in the evolvement of stapler haemorrhoidopexy. Our aim is to study the efficacy of stapler haemorrhoidopexy with regards to role of immediate post-operative morbidity. A prospective study of 50 patients (n = 50) with the second- and third-degree symptomatic haemorrhoids was done. The mean age of the patients was 44.1 years. Fourteen patients had co-morbid conditions. The average duration of the operation was 29 min. Patients with the second-degree haemorrhoids had higher rate of complication. The complication rate was 32%. Three patients had urinary retention. Two patients had minor bleeding, and one patient experienced transient discharge. The mean analgesic requirement was 2.4 tramadol, 50 mg injections. Ten patients had significant post-operative pain. Average length of hospital stay was 2.7 days. There were no symptomatic recurrences till date.

Focal seizures (also called partial seizures [citation needed] and localized seizures) are seizures which affect initially only one hemisphere of the brain. [citation needed] The brain is divided into two hemispheres, each consisting of four lobes – the frontal, temporal, parietal and occipital lobes.
Ovarian cancer warning signs include ongoing pain or cramps in the belly or back, abnormal vaginal bleeding, nausea, and bloating. Depending on the cancer stage, ovarian cancer treatment includes surgery and chemotherapy.

If it is not removed, tooth decay will begin. The acids in plaque damage the enamel covering your teeth. It also creates holes in the tooth called cavities. Cavities usually do not hurt, unless they grow very large and affect nerves or cause a tooth fracture.

Today, the most common approach for open-heart surgery is a sternotomy, which requires a 12-14-inch incision through the breastbone. But in the hands of experienced minimally invasive surgeons, many cardiac procedures can be performed through smaller 2- to 3-inch incisions between the ribs without the need to cut through the breastbone. Learn more in this medical animation from Sarasota Memorial's Minimally Invasive Cardiac Surgery Team and medical director Jonathan Hoffberger, DO. For information or referrals, visit smhheart.com.
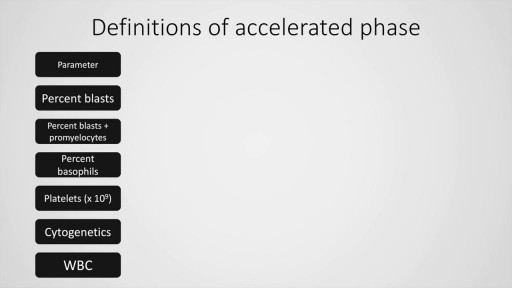
Chronic myeloid leukaemia is a common malignancy worldwide. We have come a long way from the limited treatment options and survival in this condition. Today, CML is a treatable malignancy with more than 80% patients surviving beyond 10 years after diagnosis, in absence of complications. This presentation deals with the definition, diagnostic criteria of chronic phase, accelerated and blastic phase (MD Anderson cancer centre, International bone marrow transplant registry and the WHO for the latter two) and management (first and second generation tyrosine kinase inhibitors) of this condition. Finally, a stepwise approach to chronic myeloid leukaemia is also presented including the definitive modality of treatment, allogeneic stem cell transplantation.
A ureteral stent, sometimes as well called ureteric stent, is a thin tube inserted into the ureter to prevent or treat obstruction of the urine flow from the kidney. The length of the stents used in adult patients varies between 24 to 30 cm.

This video demonstrate Laparoscopic Cholecystectomy Full Length Skin to Skin Video with Infrared Cholangiography performed by Dr R K Mishra at World Laparoscopy Hospital. Infrared Cholegiography is performed by using Indocyanine Green during laparoscopic cholecystectomy surgery for gallbladder removal. Bile duct injury remains the most feared complication of laparoscopic cholecystectomy. Intraoperative cholangiography (IOC) is the current gold standard for biliary imaging and may reduce injury, but is not widely used because of the difficulties of doing it. Near-Infrared Fluorescence Cholangiography (NIRF-C) is a novel non-invasive method for real-time, radiation-free, intra-operative biliary mapping during laparoscopic cholecystectomy. We have experienced that NIRF-C is a safe and effective method for identifying biliary anatomy during laparoscopic cholecystectomy. Indocyanine green is a cyanine dye is very popular and used for many years in medical diagnostics. It is used for determining cardiac output, hepatic function, liver, and gastric blood flow, and for ophthalmic angiography. Now the use of this dye in lap chole has improved the safety of this surgery by NEAR INFRARED FLUORESCENT CHOLANGIOGRAPHY.
For more information please contact:
World Laparoscopy Hospital
Cyber City, Gurugram, NCR DELHI
INDIA 122002
Phone & WhatsApp: +919811416838, + 91 9999677788
Pacemaker Implantation 3D Animation

Podalic version is an obstetric procedure wherein the fetus is turned within the womb such that one or both feet present through the cervix during childbirth. It is used most often in cases where the fetus lies transversely or in another abnormal position in the womb.

Reverse sural flap for ankle and heel soft tissues reconstruction
