- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Experts do not know the exact cause of Zollinger-Ellison syndrome. About 25 to 30 percent of gastrinomas are caused by an inherited genetic disorder called multiple endocrine neoplasia type 1 (MEN1). MEN1 causes hormone-releasing tumors in the endocrine glands and the duodenum.

Detailed video of Arthroscopic ACL Reconstruction using four stranded hamstring graft

Probes, landmarks, and general windows to obtain transthoracic echo views

Wondering how pregnancy happens? It’s not as simple as it seems! Pregnancy takes several days, and there are lots of steps. Here are the basics on how pregnancy works.

Exercise For Positioning Baby in Womb
What happens to our bodies after we die?

Our nervous system is involved in everything our body does, from maintaining our breath to controlling our muscles. Our nerves are vital to all we do; therefore, nerve pain and damage can heavily influence our quality of life. In Discovery News' latest video, "Why Can't We Reverse Nerve Damage?" host Lissette Padilla explains the central nervous system (CNS) has certain proteins that inhibit cell regeneration, because each cell in the nervous system has a unique function on the pathway, like a circuit, and can't be replaced.

Thousands of Whiteheads! Why Do I Get Them?

Multiple studies demonstrate the safety of propofol in pediatric EDPS. Each has identified a drop in blood pressure and transient hypoxemia as the most frequent complications. In all of the studies in which hypotension was identified there was no evidence of poor perfusion. The hypoxemia in all of these studies quickly responded to minimal intervention with no apparent lasting complications. Although these were pediatric studies, the results were very similar to ours in complication rates and sedation times. Our study did not demonstrate the frequency of decreased blood pressure seen in these pediatric studies but had similar hypoxemia rates.

If your knee is severely damaged by arthritis or injury, it may be hard for you to perform simple activities, such as walking or climbing stairs. You may even begin to feel pain while you are sitting or lying down. If nonsurgical treatments like medications and using walking supports are no longer helpful, you may want to consider total knee replacement surgery. Joint replacement surgery is a safe and effective procedure to relieve pain, correct leg deformity, and help you resume normal activities. Knee replacement surgery was first performed in 1968. Since then, improvements in surgical materials and techniques have greatly increased its effectiveness. Total knee replacements are one of the most successful procedures in all of medicine. According to the Agency for Healthcare Research and Quality, more than 600,000 knee replacements are performed each year in the United States. Whether you have just begun exploring treatment options or have already decided to have total knee replacement surgery, this article will help you understand more about this valuable procedure.

Comprehensive Cancer Center, provides definitions and terms used in cancer diagnosis and treatment. He explores the process of diagnosis from biopsies to imaging and how staging is established. He also discusses the multimodality approach to treatment which typically includes surgical oncology, medical oncology and radiation oncology. Series: "UCSF Osher Center for Integrative Medicine presents Mini Medical School for the Public
Famous Faces With Hepatitis C You share needles and other equipment used to inject illegal drugs. ... You had a blood transfusion or organ transplant before 1992. ... You get a shot with a needle that has infected blood on it. ... You get a tattoo or a piercing with a needle that has infected blood on it.

The Steri-Strip™ brand offers an extended line of adhesive skin closures to meet your needs. Our versatile, cost-saving, non-invasive Steri-Strips™ have many applications and come in a variety of sizes. Options include reinforced, elastics, "blend-tone," an antimicrobial and a waterproof wound closure system.

Smoking kills, but what exactly is smoking doing to your body that kills it?
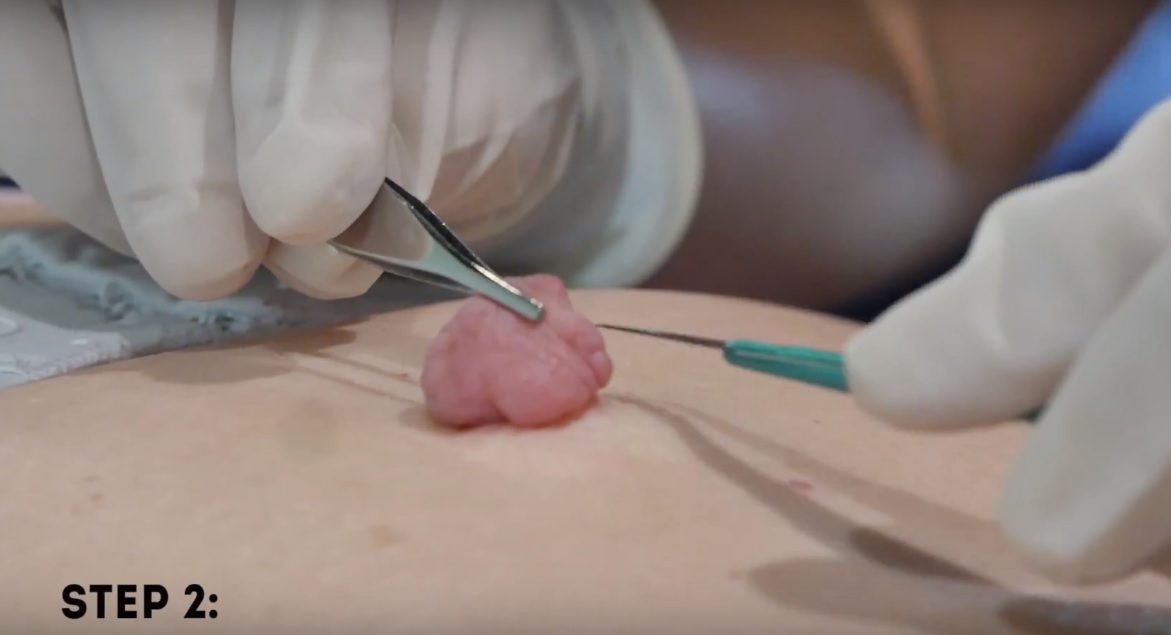
Watch that Huge Skin Tag Removal Procedure

http://eliminar-celulite.plus101.com --- Eliminar Celulite, O Que Fazer Para Acabar Com A Celulite, Como Tirar Celulite Das Pernas. Mas as razões que vou compartilhar são diferentes das que a maioria das outras fontes está tentando fazê-la acreditar. Há um mito fazendo com que algumas mulheres acreditem que certos alimentos e nutrientes irão “eliminar as toxinas que estão causando a celulite”. ISSO É TOTALMENTE FALSO, porque não há toxinas em ou sob sua pele. Se houvesse toxinas se acumulando e ficando presas sob sua pele, você estaria morta. Simples assim. Nosso corpo foi feito para remover toxinas com muita eficácia. Este processo fisiológico acontece 24 horas por dia, 7 dias por semana, sem parar, o tempo todo. Então, a ideia não comprovada de que “toxinas” são a causa de sua celulite significa que a celulite não pode ser revertida ao “eliminá-las” com alguns alimentos, porque elas não estão lá, para começar. Mas não se preocupe, porque eis o que o planejamento alimentar apropriado pode fazer para reverter, ou prevenir, a raiz da causa da celulite em suas pernas, bumbum, quadris e coxas. Uma verdadeira dieta contra a celulite fornece nutrientes em quantidades que impactam positivamente a regulagem e equilíbrio dos hormônios femininos. Esta é a razão principal de o Planejamento Alimentar/Dieta Contra Celulite do "Adeus Celulite" só estar disponível para mulheres que começam com o Método de Exercícios SYMULAST do programa Adeus Celulite. Então se você estiver interessada, vá para: http://eliminar-celulite.plus101.com

Watch that video of human Fetus Removal Surgery

Watch that video of Unreal Mutations and Medical Condition

Pulling pins out of the leg
