- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Harvard Plastic Surgery
Mohamed
867 Views • 3 years ago
n,n,n,mm

Thailand's Emergency Care
ThailandMedical Tourism
9,793 Views • 3 years ago
Thailand has top-notch, fast and efficient emergency care
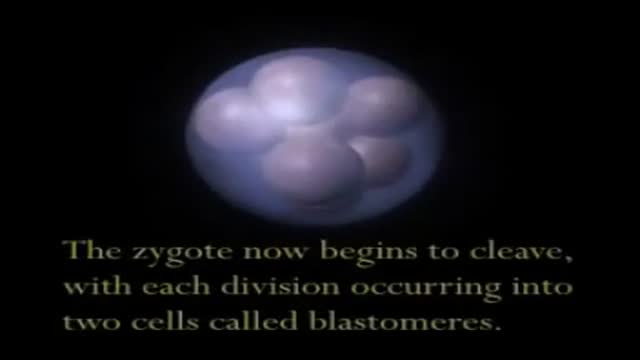
Embryo and Fetal Development
Doctor
10,648 Views • 3 years ago
A video showing Embryo and Fetal Development
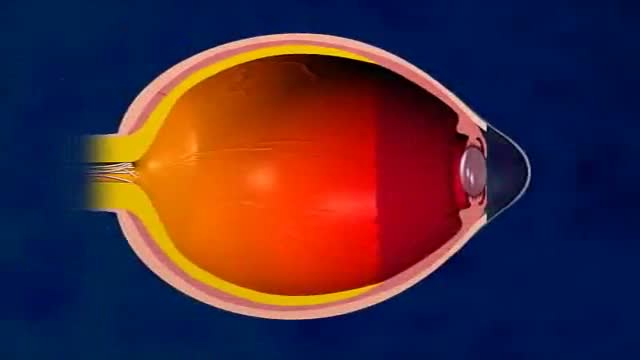
LASIK Eye Surgery 3D Animation
Scott Stevens
6,679 Views • 3 years ago
LASIK Eye Surgery 3D Animation

Ingrown Toenail Surgery HD
Scott Stevens
19,394 Views • 3 years ago
Ingrown Toenail Surgery HD

Galant Reflex
Medical_Videos
7,425 Views • 3 years ago
Galant Reflex

Histology of Hyaline Cartilage
Histology
4,716 Views • 3 years ago
Histology of Hyaline Cartilage

Histology of Fibrocartilage
Histology
4,434 Views • 3 years ago
Histology of Fibrocartilage
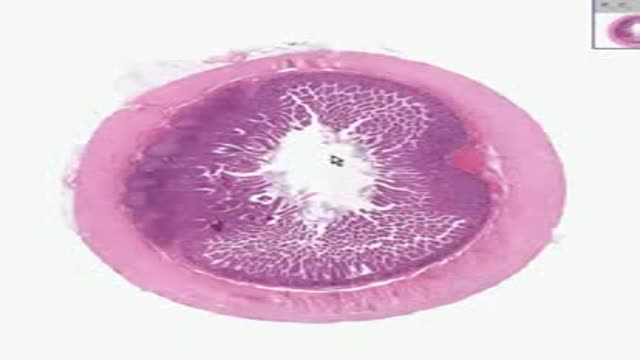
Histology of Small Intestine Illeum
Histology
6,577 Views • 3 years ago
Histology of Small Intestine Illeum
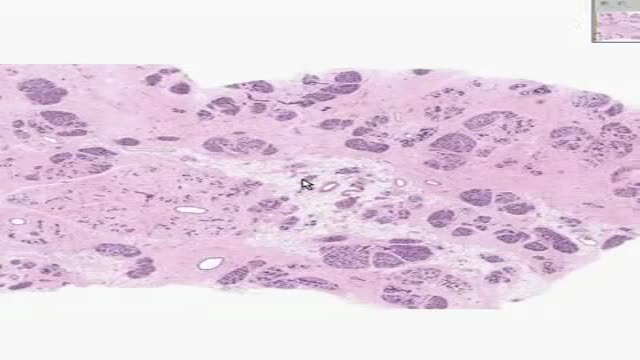
Histology of Inactive Breast
Histology
7,076 Views • 3 years ago
Histology of Inactive Breast

Intramuscular Injection Technique
Harvard_Student
11,837 Views • 3 years ago
Intramuscular Injection Technique

Thoracocentesis Removing 1200CC Pleural Fluid
Harvard_Student
9,035 Views • 3 years ago
Thoracocentesis Removing 1200CC Pleural Fluid
ABG How to Analyze
Harvard_Student
6,989 Views • 3 years ago
ABG How to Analyze

Drugs Through a Saline Lock
Harvard_Student
6,792 Views • 3 years ago
Drugs Through a Saline Lock

qatar liposuction clinics
dr. kamal hussein saleh al husseiny
1,122 Views • 3 years ago
qatar liposuction clinics
Problem Behaviors
Scott
5,606 Views • 3 years ago
Problem Behaviors

Plantar Fascia Release
Anatomist
8,793 Views • 3 years ago
Plantar Fascia Release

Foramen Magnum Neurofibroma Video
Anatomist
7,249 Views • 3 years ago
Foramen Magnum Neurofibroma Video

Abnormal Eye Lid Positions Ptosis
Alicia Berger
6,566 Views • 3 years ago
Abnormal Eye Lid Positions Ptosis
3D MRI of Human Brain
Scott
9,080 Views • 3 years ago
3D MRI of Human Brain
Showing 343 out of 373
