- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Plantar Fascia Release

Foramen Magnum Neurofibroma Video

Abnormal Eye Lid Positions Ptosis
3D MRI of Human Brain

High Blood Pressure Body Effects

ECG Leads Placement

http://www.landging.com/car-crash-animations-rear.html
Car crash animations, accident reconstruction, rear end collision.

http://www.landging.com/animated-city.html
420 seconds 3d animation which is developed for Expo 2010 Shanghai Aviation Pavilion and demonstrates an animated city.

visit https://www.facebook.com/medical.hint
to check the answers
Health disorders are part of life when you are getting older , Some problems are life-threatening, while others lower the quality of life. The good news is that these Health disorders can be managed effectively.
homecareassistancesouthjersey.com
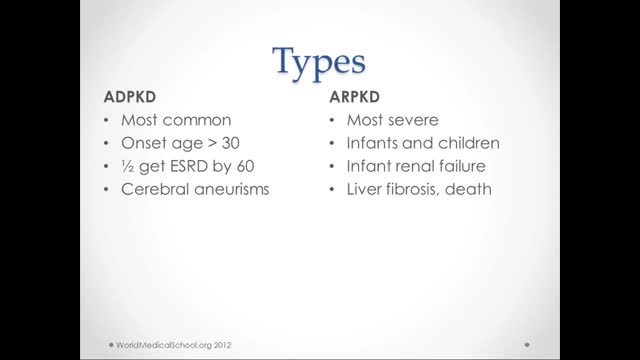
What is polycystic kidney disease? Polycystic kidney disease (also called PKD) causes numerous cysts to grow in the kidneys. These cysts are filled with fluid. If too many cysts grow or if they get too big, the kidneys can become damaged. PKD cysts can slowly replace much of the kidneys, reducing kidney function and leading to kidney failure. How common is PKD? In the United States about 600,000 people have PKD. It is the fourth leading cause of kidney failure. It is found in all races and occurs equally in men and women. It causes about 5% of all kidney failure. What other organs besides the kidney are affected by PKD? PKD can affect other organs besides the kidney. People with PKD may have cysts in their liver, pancreas, spleen, ovaries, and large bowel. Cysts in these organs usually do not cause serious problems, but can in some people. PKD can also affect the brain or heart. If PKD affects the brain, it can cause an aneurysm. An aneurysm is a bulging blood vessel that can burst, resulting in a stroke or even death. If PKD affects the heart, the valves can become floppy, resulting in a heart murmur in some patients. What are the clues that someone has PKD? Most people do not develop symptoms until they are 30 to 40 years old. The first noticeable signs and symptoms may include: Back or side pain An increase in the size of the abdomen Blood in the urine Frequent bladder or kidney infections High blood pressure High blood pressure is the most common sign of PKD. Occasionally, patients may develop headaches related to high blood pressure or their doctors may detect high blood pressure during a routine physical exam. Because high blood pressure can cause kidney damage, it is very important to treat it. In fact, treatment of high blood pressure can help slow or even prevent kidney failure. Fluttering or pounding in the chest About 25% of PKD patients have a so-called floppy valve in the heart, and may experience a fluttering or pounding in the chest as well as chest pain. These symptoms almost always disappear on their own but may be the first hint that someone has PKD. How is PKD diagnosed? Ultrasound is the most reliable, inexpensive and non-invasive way to diagnose PKD. If someone at risk for PKD is older than 40 years and has a normal ultrasound of the kidneys, he or she probably does not have PKD. Occasionally, a CT scan (computed tomography scan) and MRI (magnetic resonance imaging) may detect smaller cysts that cannot be found by an ultrasound. MRI is used to measure and monitor volume and growth of kidneys and cysts. In some situations, genetic testing might also be done. This involves a blood test that checks for abnormal genes that cause the disease. Genetic testing is not recommended for everyone. The test is costly, and it also fails to detect PKD in about 15% of people who have it. However, genetic testing can be useful when a person: has an uncertain diagnosis based on imaging tests has a family history of PKD and wants to donate a kidney is younger than 30-years old with a family history of PKD and a negative ultrasound, and is planning to start a family
Friedreich's ataxia is an inherited disease that damages your nervous system. The damage affects your spinal cord and the nerves that control muscle movement in your arms and legs. Symptoms usually begin between the ages of 5 and 15. The main symptom is ataxia, which means trouble coordinating movements. Specific symptoms include Difficulty walking Muscle weakness Speech problems Involuntary eye movements Scoliosis (curving of the spine to one side) Heart palpitations, from the heart disease which can happen along with Friedreich's ataxia People with Friedreich's ataxia usually need a wheelchair 15 to 20 years after symptoms first appear. In severe cases, people become incapacitated. There is no cure. You can treat symptoms with medicines, braces, surgery, and physical therapy.

10 Strange Scientific Facts About Your Body During Sex

Baby Survives Being Born Twice:
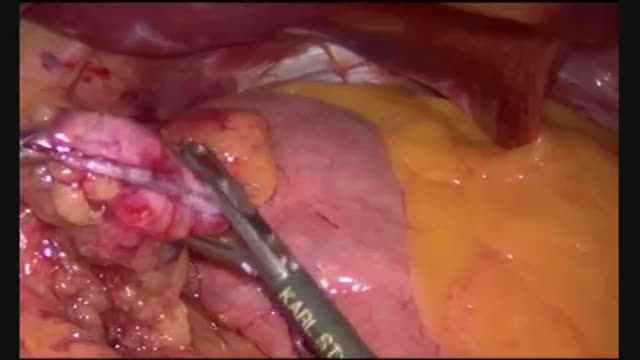
Gastric Bypass Surgery - Maagverkleining - Weight Loss Surgery - WLS
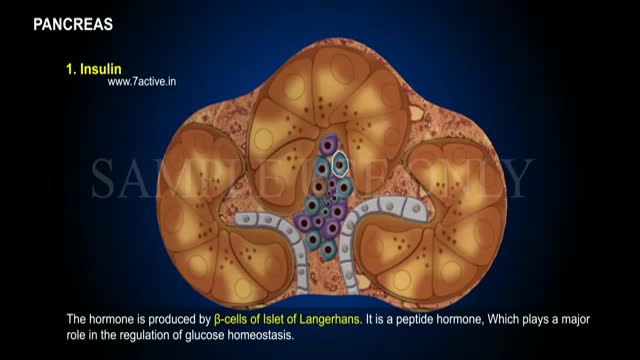
Enzymes, or digestive juices, produced by the pancreas are secreted into the small intestine to further break down food after it has left the stomach. The gland also produces the hormone insulin and secretes it into the bloodstream in order to regulate the body's glucose or sugar level.

Peritoneal dialysis is a treatment for kidney failure that uses the lining of your abdomen, or belly, to filter your blood inside your body. ... The process of first draining the used dialysis solution and then replacing it with fresh solution is called an exchange.

Dextrocardia situs inversus refers to the heart being a mirror image situated on the right side. For all visceral organs to be mirrored, the correct term is dextrocardia situs inversus totalis. Dextrocardia is believed to occur in approximately 1 in 12,000 people.

Such foods include carrots, eggplant, cauliflower, green beans, broccoli, peppers, onions, lettuce, zucchini, tomatoes, peanuts and walnuts. These foods are generally safe for you to eat at each meal without spiking your blood sugar.

Intelligent People Have Fewer Friends, Here's Why...
