- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
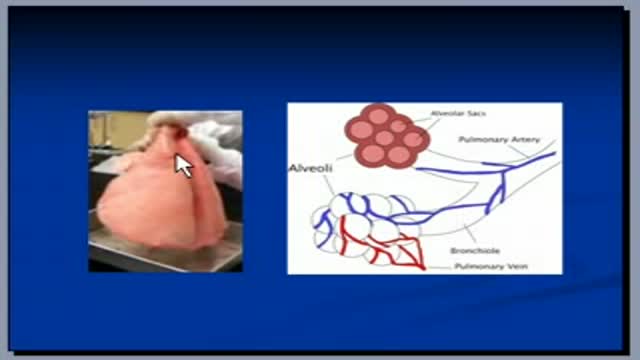
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
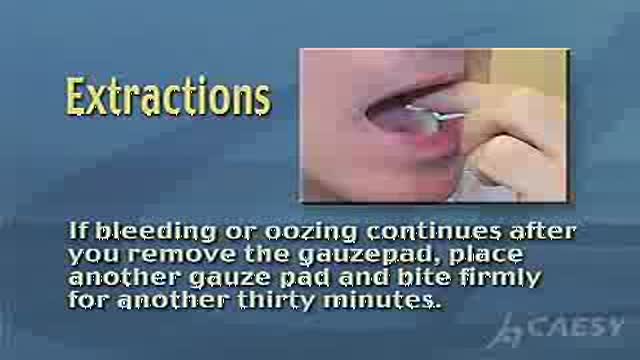
Hemostasis after Tooth Extraction

Infant CPR Video Demonstration
The video will help you to understand radiologic anatomy. Please see my website for disclaimer.

Muscle Biopsy
A discussion and demonstration of suturing techniques with Lee Dresang, MD from the University of Wisconsin Department of Family Medicine

This podcast, intended for the general public, demonstrates how to put on and take off disposable respirators that are to be used in areas affected by the influenza outbreak.

This video is demonstrating the Interscalene Block Video

Bat Ears Correction Plastic Surgery

The video will describe pneumomediastinum on a chest x-ray. Please see disclaimer on my website www.academyofprofessionals.com

Uterus removed from patient with longstanding fibroid
Demonstration of Ballon Stent Surgery
الدكتور إياس الموسى من عمان، الاردن، يتحدث عن خفقان القلب، ما هي أعراضه، أسبابه وكيفية علاجه.
العديد من الأسئلة التي ترد إلى موقع الطبي تتعلق بخفقان وتسارع القلب. الدكتور إياس يشرح بإسهاب عن هذه المشكلة السائدة

bnbmedispa.com offers Titan Laser, Zerona Laser, Zerona Laser Treatment, Titan skin tightening in NJ, Monmouth, and Shrewsbury. call us at (732) 460-0600 to get discout on any laser treatment.
WORLD`S BEST IMMEDIATE ZIRCONIA DENTAL IMPLANT SOLUTION video
A tutorial showing ascending sensory pathways

Laparoscopy by Dr. Emadi in Qatar

Posterior Iris Claw Lens Implantataion

Ingrown Toenail Surgery HD

Short Leg Cast
Beating Coronary Heart Surgery
