Los mejores videos

3D printing a titanium vertebrae

the elbow is the second most frequently dislocated major joint, after the shoulder. It is the most commonly dislocated joint in children. [1] More than 90% of all elbow dislocations are posterior dislocations. This injury entails disengagement of the coronoid process of the ulna from the trochlea of the humerus with movement posteriorly. [2] The mechanism of injury is typically a fall onto an outstretched hand (FOOSH) with the elbow in extension upon impact.
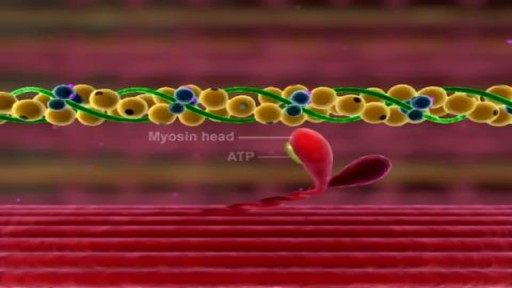
Muscle Contraction Part 3 The Cross Bridge Cycle

A pacemaker insertion is the implantation of a small electronic device that is usually placed in the chest (just below the collarbone) to help regulate slow electrical problems with the heart.

Gallbladder & Gallstone Removal Surgery
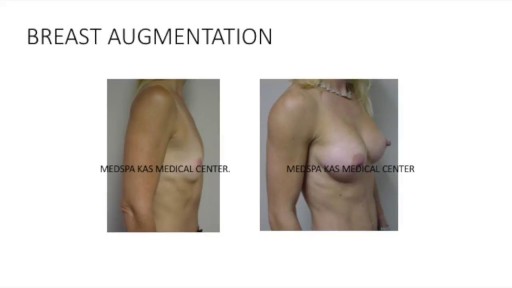
This is a complete video of breast augmentation procedure with implants also includes some before after photographs of breast augmentation surgery by Dr. Ajaya Kashyap at MedSpa Clinic, Delhi, India. source: https://www.youtube.com/watch?v=tRg3RkvCvOE Get more information: www.bestbreastsurgeryindia.com Get more information: www.themedspa.us Email at: info@themedspa.us Call/WhatsApp on:+91-9818369662, 9958221983/82/81

Watch that video to know the Serious Side Effects of Steroids on The Human Body

Watch that video of Horrible Skin Jiggers Removal

Que Es Bueno Para La Impotencia Del Hombre, Problemas Para Mantener La Erección, Que Es Erección.--- http://erecciones-increibles.good-info.co --- 5 Errores comunes que empeoran tu disfunción eréctil, Cuando se trata de problemas de salud, a menudo somos nuestros peores enemigos. Esto se ve en muchos casos y con una variedad de enfermedades. Las personas que saben que tienen la presión arterial elevada y colesterol alto no cambian su dieta y siguen comiendo un montón de comida frita, por ejemplo. La disfunción eréctil no es diferente. Aquí hay cinco cosas que podrías estar haciendo en este momento, hoy, que están empeorando tu estado. Estás comiendo (y bebiendo) cosas malas Cafeína. Alcohol. Nicotina. Drogas. Exceso de grasa. Si disfrutas de cualquiera de estas cosas habitualmente, la triste verdad es que estás empeorando tu disfunción eréctil. Incluso si haces otras cosas para mejorar tu estado - incluso si tomas medicación para compensarlo, esas cosas serán menos eficaces de lo que podrían ser a menos que reduzcas dramáticamente o elimines los ítems mencionados anteriormente. No estás comiendo suficiente cosas buenas A continuación se presenta una corta lista de alimentos para aumentar tu salud vascular, lo que a su vez, mejorará la calidad de tus erecciones: granos enteros, verduras de hojas verdes, frutas (especialmente la sandía y arándanos), y ostras. Si te gusta todo lo de esa lista, estás de suerte. Come más de todo eso y vas a ver que los síntomas de la disfunción eréctil disminuyen considerablemente, y posiblemente incluso desaparezcan. Si actualmente no estás comiendo ninguno de los anteriormente, entonces definitivamente estás empeorando el problema. En sí misma, la dieta puede no ser completamente capaz de curar tu disfunción eréctil, pero puede hacer una gran diferencia y tener un tremendo impacto en la calidad de tus erecciones. Esta es la única cura comprobada para la disfunción eréctil que es 100% segura y natural, y combina un secreto ancestral de los amantes más viriles del mundo con ciencia moderna y revolucionaria… Ingresa ahora a: http://erecciones-increibles.good-info.co

Watch that video to see how black salve left inch-wide hole in man's face

Iodine For Ringworm, Best Ointment For Ringworm, Where Do You Get Ringworm, How To Treat Ring Worms ---- http://ringworm-cure.plus101.com --- Ringworms, contrary to the common notion, do not come from worms. Tinea, which is the medical term for ringworms, is a fungal infection seen on the skin's surface. Knowing how to cure ringworm is important because ringworms can be highly contagious. It can be contracted from direct contact with the host (person or animal) as well as by other means such as having contact with the host's clothes. Swimming pools can also be a place where ringworms are transmitted from one person to another. How To Cure Ringworm - Understanding Aspects and Options Different means on how to cure ringworm are available and they sometimes vary in accordance with where the ringworm is located (it can appear in areas like the nails, fingers, toes, feet, scalp, stomach, chest, thighs, and scalp), and the particular type of ringworm. • Ringworms found in the scalp are usually treated with an antifungal shampoo to keep the area dry and clean. • Ringworms found in the feet can be treated through the application of ointments. • Oral medications can also be taken in especially when ringworms are on the nails. • Sprays, powders and creams are also forms by which anti-fungal drugs are bought. These medicines may take some time to work. The infection may persist for a few weeks to several months, depending on the severity and how the body responds to the medications. How To Cure Ringworm - OTC and Prescription Medications Ringworm appears on the skin's surface as an itchy, red, circular patch. As it progresses, it expands and smaller round patches can develop. It is important to immediately identify ringworms and know how to treat them properly. There are many over the counter topical creams (anti-fungal ones) and ointment that can be bought in the market. However, some people prefer to visit the doctor and ask for a prescription. Stronger formulations are generally available via prescriptions. William Oliver is a nutritionist, medical researcher, and author of the Fast Ringworm Cure e-book. To find out how to cure Ringworm in 3 days or less, click below: http://ringworm-cure.plus101.com

Video demonstrates the fundamental components of placing your first suture.

Split Skin Graft

How to Prepare, Apply & Remove a Total Contact Cast

How Did Insects Evolve To Feast On Your Blood?

This is the first video of 5, where Mike teamed up with Graham from On Your Marks Fitness and Coaching to show us some exercises to strengthen our muscles, and improve our soccer game! Make sure your feet are planted safely or held by a friend, and keep your back straight, and over your knees. Use the swiss ball to keep you steady, and SQUEEZE those muscles! Check us out on Social Media! Facebook: https://www.facebook.com/striveptandperformance/ Instagram: https://www.instagram.com/striveptandperf/ Twitter: https://twitter.com/StrivePTandPerf Blog: http://www.strivept.ca/blog

Robotic Surgery Demonstration Using Da Vinci Surgical System
Like a fine whiskey barrel and wine cellar, cannabis also comes at its best when aged in a dark, cool place. Though there is no steadfast expiration date for cannabis, the method you use for preserving the cannabis makes a big difference in maintaining the buds’ freshness and potency. The question is, how do you store cannabis in a way that could extend its longevity while maintaining the vigor and freshness? Experts have described different methods. However, here are some time-proven methods that are easy and inexpensive and require very less equipment. Use air-tight glass containers to store the weed Use clean air-tight glass containers or jars to store cannabis. You can buy glass containers from any ordinary supermarket or hardware store. The tricky part is to make sure you do leave some air in the container while the air stored with cannabis isn’t in detrimental extent. Always leave 1/4 space at the top of the canister or container. Do not fill the containers to the brim with the buds. If you leave no air, then the buds will dry out. If you have too much air, the buds will get damp and moldy. Freeze your cannabis in a convenient temperature The best way to store your buds is in air-tight glass jars, in a cool and dark place under an ideal temperature between 60 and 70 degrees Fahrenheit. If you need to store a high volume of cannabis, you can freeze them after keeping them completely dry for a period of 4 weeks. On this note, you should know that you must not handle frozen buds until it becomes normal in room temperature as trichomes become brittle and can easily break off in freezing temperature. Refrigerate your cannabis (Not Recommended) Even if you use airtight jars, cannabis can grow mold in the fridge. So, you should avoid storing cannabis in the fridge. If you can’t help but doing it, make sure the weed is completely dry and put them in the back where the humidity and temperature don’t fluctuate. Plastic Baggies (Worst method!) Albeit this is very common among people who aren’t expert in handling cannabis, this is the worst of all storage methods. Cannabis gets brittle and dries out in plastic bags. It also loses its natural smell, and the potency deteriorates sharply. So, it should be avoided entirely or can be used for a short-term if there is no better alternative. Here are some things you should know while storing cannabis - Make sure cannabis has been cured for at least 4 weeks before putting them into long-term storage. Without proper curing before storage, the buds can lose their strength and smoothness. - Sunlight can stop the medicinal qualities of cannabis. Your cannabis, if stored correctly, can maintain its medicinal qualities for a few years. Exposure to Sun will turn your cannabis brown, no matter how you have stored it away. - Air-tight, nonporous glass jar are the best way for storing the buds for long term. You can use metal or plastic box/bag, but that could reduce the smell and taste after a while. - Avoid heat and middling temperature in the place where you store your buds. The ideal temperature is 60-70°F (15-21°C) or under 32°F (0°C). Extra heat, cold or middling temperature cause the cannabis potency to decrease. - Keep your cannabis away from any electronic devices or appliances that will expose the cannabis to heat. Keeping cannabis on top of a microwave, or near a laptop or mobile charge is a bad idea. Now, as you know that how to store cannabis properly and make it last for years, enjoy the best form of your weeds even it comes from the previous year. Do write to us in the comments section if you have any questions. Also, don’t forget to hit the subscribe button below. Visit OnlineMedicalCard.com now to get an MMJ recommendation online in less than 10 minutes.
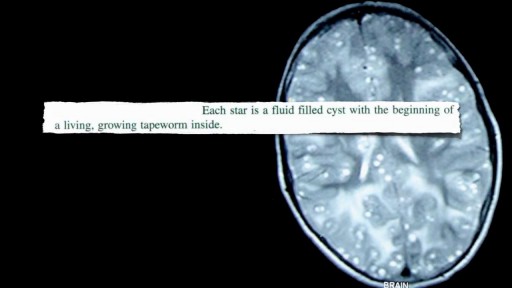
Neurocysticercosis Pork Worms Infecting Human Brain
