- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
How To Get Pregnant, Ways To Get Pregnant, Best Days To Get Pregnant, Easiest Way To Get Pregnant.
http://how-to-get-pregnant.info-pro.co
Signs Of Infertility
What Exactly Is Infertility?
The problems with either conceiving a child, or with carrying out the pregnancy to its eventual fruitful end, fall under the definition of infertility. Infertility is the incapability of an individual to become pregnant, in case of females, or the incapability to induce pregnancy, in case of the males.
The inability of an individual to carry out a pregnancy to its full term is also dubbed infertility. How does one recognize infertility? What are the signs of infertility?
Signs of infertility in women:
Children At Age 43 After Years Of "Trying".
You Can Too! Here's How...": http://how-to-get-pregnant.info-pro.co
For More Information
http://how-to-get-pregnant.info-pro.co
http://natural-fertility-remedies.blogspot.com/
Subscribe To Our Channel
https://www.youtube.com/watch?v=R6gRskH4WxY
How To Get Pregnant, Ways To Get Pregnant, Best Days To Get Pregnant, Easiest Way To Get Pregnant, preparing for pregnancy, pills to get pregnant, tricks for getting pregnant, help with pregnancy, help me get pregnant faster, how you get pregnant fast, i really want to get pregnant, male infertility treatments, get me pregnant, natural tips to get pregnant, tips on getting pregnant, how to help get pregnant faster
Alimentos Para Controlar La Presion Arterial, Arterial Hypertension, Prevencion De Hipertension
http://bajar-presion-arterial.good-info.co
Para obtener los mismos beneficios que los medicamentos prescritos más comúnmente
sin los efectos secundarios negativos existen alternativas naturales. La dieta es la principal manera de aumentar las reacciones deseables, pero el ejercicio contribuye en gran medida también.
Por ejemplo, la misma reacción causada por los vasodilatadores puede ocurrir cuando usted obtiene suficiente L-Arginina. Este aminoácido permite que las paredes de los vasos sanguíneos se relajen. Usted puede tomar un suplemento o conseguirla a través de proteínas de origen animal, el maní y la soja.
http://bajar-presion-arterial.good-info.co
https://www.youtube.com/watch?v=SFUGz4IqbA0
Alimentos Para Controlar La Presion Arterial, Arterial Hypertension, Prevencion De Hipertension, Arterial Pdf, Hipertension Esencial, Hipertension Pulmonar Tratamiento,Tension Alta Sintomas, Dieta Hipertension, Guia Clinica Hipertension, Sal Marina Hipertension,
Sintomas De Tension Alta, Hipertension Portal Pdf, Hipertension Arterial Clasificacion, Hipertension Intracraneal, Tension Alta En, El Embarazo, Hipertension Primaria

Vaginale pijn behandelen met amitriptyline creme. Vulvodynia is een groot probleem en komt (onuitgesproken) bij veel vrouwen voor. Wij hebben enkele topicale cremes ontwikkeld, waaronder een amitriptyline-palmnitoylethanolamide en een baclofen-palmitoylethanoamide creme, waar veel vrouwen veel baat bij hebben.
Check out how Physician Coder – an online specialty solution – can help you meet your practice’s goals for error-free coding. From helping you meet all your ICD-10 coding needs from one place with code lookup, crosswalk, superbill converter, scrubber, and monthly specialty articles to helping you review CPT® 2016 changes with expert analysis for your specialty, we have you covered. Plus, you’ll also learn how to stay up-to-date on 2016 fee schedule details like RVUs, global days, and MUEs; check the latest CCI edits and view LCD policy details.
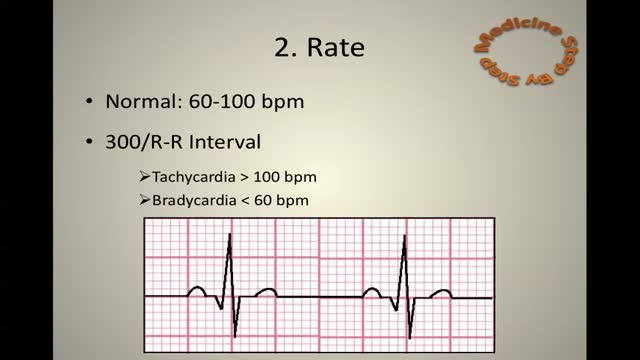
ECG Learn it
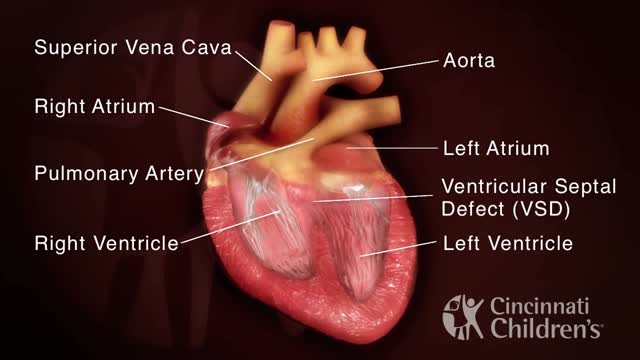
Tetralogy of Fallot (teh-TRAL-uh-jee of fuh-LOW) is a rare condition caused by a combination of four heart defects that are present at birth. These defects, which affect the structure of the heart, cause oxygen-poor blood to flow out of the heart and to the rest of the body. Infants and children with tetralogy of Fallot usually have blue-tinged skin because their blood doesn't carry enough oxygen. Tetralogy of Fallot is often diagnosed during infancy or soon after. However, tetralogy of Fallot might not be detected until later in life, depending on the severity of the defects and symptoms. With early diagnosis followed by appropriate surgical treatment, most children who have tetralogy of Fallot live relatively normal lives, though they'll need regular medical care and might have restrictions on exercise.

Atopic dermatitis (eczema) is a condition that makes your skin red and itchy. It's common in children but can occur at any age. Atopic dermatitis is long lasting (chronic) and tends to flare periodically and then subside. It may be accompanied by asthma or hay fever.
Rapid Algorithm Review Ventricular Fibrillation

Can the flu be treated? Yes. There are prescription medications called “antiviral drugs” that can be used to treat flu illness. What are antiviral drugs? Antiviral drugs are prescription medicines (pills, liquid, an inhaled powder, or an intravenous solution) that fight against the flu in your body. Antiviral drugs are not sold over-the-counter. You can only get them if you have a prescription from your doctor or health care provider. Antiviral drugs are different from antibiotics, which fight against bacterial infections. What should I do if I think I have the flu? If you get the flu, antiviral drugs are a treatment option. Check with your doctor promptly if you are at high risk of serious flu complications (see box below for the full list of high risk factors). Flu symptoms can include fever, cough, sore throat, runny or stuffy nose, body aches, headache, chills and fatigue. Your doctor may prescribe antiviral drugs to treat your flu illness. Should I still get a flu vaccine? Yes. Antiviral drugs are not a substitute for getting a flu vaccine. While flu vaccine can vary in how well it works, a flu vaccine is the first and best way to prevent seasonal influenza. Antiviral drugs are a second line of defense to treat the flu (including seasonal flu and variant flu viruses) if you get sick.

Abnormally Large Knee (part 1) - Bizarre ER
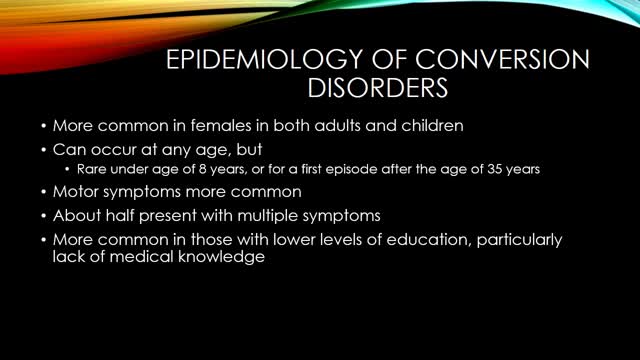
Conversion disorder, also called functional neurological symptom disorder, is a condition in which you show psychological stress in physical ways. The condition was so named to describe a health problem that starts as a mental or emotional crisis — a scary or stressful incident of some kind — and converts to a physical problem.
A hemangioma (he-man-jee-O-muh) is a birthmark that most commonly appears as a rubbery, bright red nodule of extra blood vessels in the skin. A hemangioma grows during the first year of life, and then recedes over time. A child who had a hemangioma during infancy usually has little visible trace of the growth by age 10.
Kidney failure and transplant options One of the most serious complications of polycystic kidney disease is kidney failure. This is when the kidneys are no longer able to filter waste products, maintain fluid balance, and maintain blood pressure on their own. When this occurs, your doctor will discuss options with you that may include a kidney transplant or dialysis treatments to act as artificial kidneys. If your doctor does place you on a kidney transplant list, there are several factors that determine your placement. These include your overall health, expected survival, and time you have been on dialysis. It’s also possible that a friend or relative could donate a kidney to you. Because people can live with only one kidney with relatively few complications, this can be an option for families who have a willing donor. The decision to undergo a kidney transplant or donate a kidney to a person with kidney disease can be a difficult one. Speaking to your nephrologist can help you weigh your options. You can also ask what medications and treatments can help you live as well as possible in the meantime. According to the University of Iowa, the average kidney transplant will allow kidney function from 10 to 12 years.
HAPPY THANKSGIVING
Myelodysplastic syndromes are a group of cancers in which immature blood cells in the bone marrow do not mature or become healthy blood cells. In a healthy person, the bone marrow makes blood stem cells (immature cells) that become mature blood cells over time.Aug 12, 2015
High Resolution Upper Airway Anatomy
Asthma and COPD

What Happens When You're In a Coma?

Narcolepsy is a chronic sleep disorder characterized by overwhelming daytime drowsiness and sudden attacks of sleep. People with narcolepsy often find it difficult to stay awake for long periods of time, regardless of the circumstances. Narcolepsy can cause serious disruptions in your daily routine. Sometimes, narcolepsy can be accompanied by a sudden loss of muscle tone (cataplexy) that leads to weakness and loss of muscle control. Cataplexy is often triggered by a strong emotion, most commonly laughter. Narcolepsy is a chronic condition for which there's no cure. However, medications and lifestyle changes can help you manage the symptoms. Support from others — family, friends, employer, teachers — can help you cope with narcolepsy.
How to make your loved ones feel good and happy
