- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
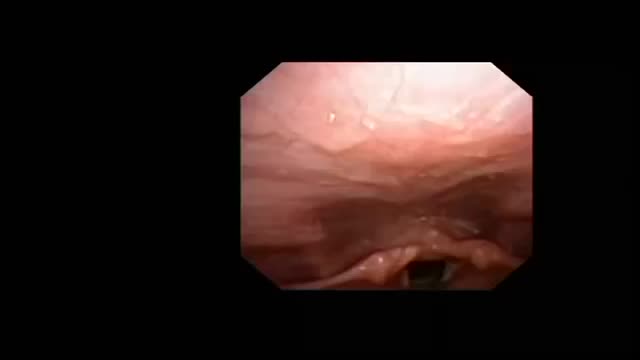
High Resolution Upper Airway Anatomy
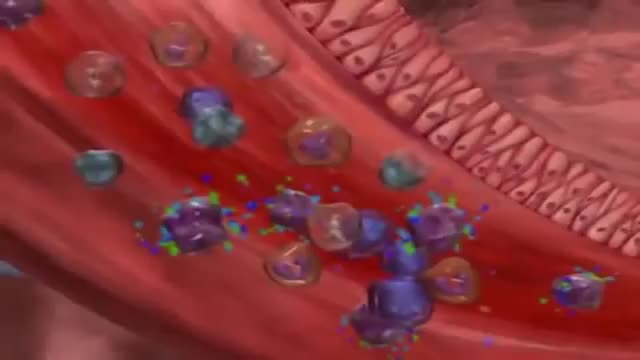
Asthma and COPD

What Happens When You're In a Coma?

Narcolepsy is a chronic sleep disorder characterized by overwhelming daytime drowsiness and sudden attacks of sleep. People with narcolepsy often find it difficult to stay awake for long periods of time, regardless of the circumstances. Narcolepsy can cause serious disruptions in your daily routine. Sometimes, narcolepsy can be accompanied by a sudden loss of muscle tone (cataplexy) that leads to weakness and loss of muscle control. Cataplexy is often triggered by a strong emotion, most commonly laughter. Narcolepsy is a chronic condition for which there's no cure. However, medications and lifestyle changes can help you manage the symptoms. Support from others — family, friends, employer, teachers — can help you cope with narcolepsy.
How to make your loved ones feel good and happy

For education, Microsoft HoloLens will help make incredible leaps forward in productivity, collaboration, and innovation. See how Microsoft HoloLens transforms the way we teach anatomy and our understanding of the human body as we help to prepare the next generation of doctors.

32 weeks pregnant, your baby has now nails on the toes and fingers. Watch this video to get detailed information of baby's development during this 33 week of pregnancy,

Questo Video 3D illustra la tecnica della Microlipocavitazione: sistema chirurgico ad ultrasuoni per ottenere l'emulsione del grasso in eccesso da eliminare. La Microlipocavitazione è una tecnica di chirurgia ambulatoriale, che richiede una modesta anestesia locale con un recupero delle proprie attività pressoché immediato.

Premature Baby's Brief Life Touches Many Others
Robotic Mitral Valve Repair

Dental Abscess extending into Submandibular space

Amazing Tattoos That Turn Scars Into Works Of Art
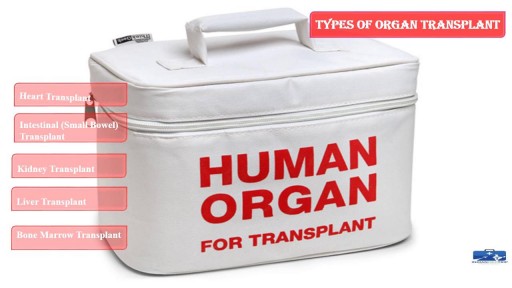
This process involves surgical removing of an #organ or tissue from one person (organ donor) & placing into another person (recipient) body. https://goo.gl/JfoN8y

http://vencer-la-diabetes-rapido.info-pro.co/ Como Controlar La Diabetes Tipo 2 Naturalmente Sin Medicamentos, Pre Diabetes Y Diabetes Tipo 1. https://youtu.be/BOSkQ5MnjT0 Que es la Insulina? Una definición practica sin adentrarnos en terminos estrictamente medicos es que la insulina es una hormona formada por 51 aminoácidos. Dentro del páncreas, las células beta producen la hormona llamada insulina. Con cada comida, las células beta liberan insulina para ayudar al cuerpo a utilizar o almacenar en la sangre la glucosa que se obtiene de los alimentos. Su déficit provoca la diabetes mellitus y su exceso provoca hiperinsulinismo con hipoglucemia. En las personas con diabetes tipo 1, el páncreas no produce insulina. Las células beta han sido destruidas y se necesitan inyecciones de insulina para utilizar la glucosa de las comidas. Las personas con diabetes tipo 2 producen insulina, pero sus cuerpos no responden bien a la misma. Algunas personas con diabetes tipo 2 necesitan medicamentos para la diabetes o inyecciones de insulina para ayudar a su cuerpo a utilizar la glucosa para obtener energía. * La insulina no se puede tomar como una píldora, ya que se descompone durante la digestión al igual que la proteína en los alimentos. Se debe inyectar en la grasa debajo de la piel para que llegue a la sangre. Existen diferentes tipos de insulina en función de la rapidez con que trabajan, y en funcion de su duración. La insulina viene en diferentes concentraciones, la más común es U-100. Tipos de insulina: * De Acción Rápida: Comienza a trabajar unos 15 minutos después de la inyección, con picos en aproximadamente 1 hora, y continúa trabajando por un tiempo de 2 a 4 horas. Tipos: Insulina glulisina (Apidra), la insulina lispro (Humalog) y la insulina aspart (NovoLog). * Regular o de Acción Corta: Generalmente llega al torrente sanguíneo a los 30 minutos después de la inyección, picos de entre 2 a 3 horas después de la inyección, y es efectiva durante aproximadamente 3 a 6 horas. Tipos: Humulin R, Novolin R * De Acción Intermedia: Generalmente llega al torrente sanguíneo de aproximadamente 2 a 4 horas después de la inyección, picos de 4 a 12 horas y eseficaz durante aproximadamente 12 a 18 horas. Tipos: NPH (Humulin N, Novolin N) * De Acción Prolongada: Alcanza el torrente sanguíneo varias horas después de la inyección y tiende a disminuir los niveles de glucosa de manera bastante uniforme durante un período de 24 horas. Tipos: La insulina detemir (Levemir) y la insulina glargina (Lantus) Nota: Esta información debes consultarla siempre con tu medico especialista. La insulina Tiene 3 Características: El inicio: Es el tiempo antes de que la insulina alcance el torrente sanguíneo y se inicie la reducción de la glucosa en sangre. Pico: Es el tiempo durante el cual la insulina está surtiendo el máximo efecto en términos de reducción de la glucosa en sangre. La duración: Es cuánto tiempo la insulina continúa reduciendo la glucosa sanguínea.
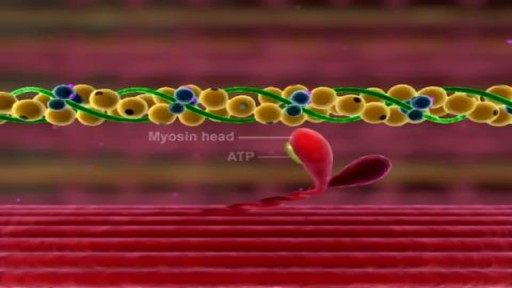
Muscle Contraction Part 3 The Cross Bridge Cycle

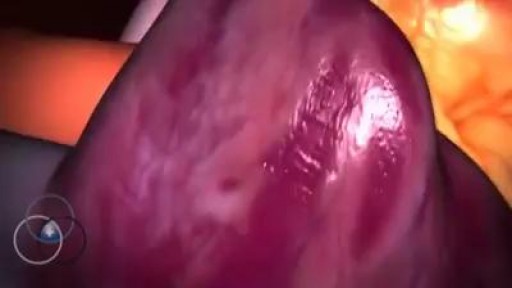
Watch that video of A Big Size Fibrodenoma Removal Surgery

baby wrapping
How To Increase Memory Power, How To Improve Memory Retention, How To Boost Memory Power.--- http://brain-revitalizer.info-pro.co ---- Brain Exercises, When people think of exercising it often involves physical exertion to strengthen muscles. The human brain is also an important "muscle" in the body and with the right brain training and brain exercises you can help keep your mind fit, alert and ready to handle the rigors of a typical working day. Often brain exercises come in the form of games that help train the brain improve memory, strategize and think in advance. Some common forms of brain exercise include chess, memory games and mathematical problem solving. Another way to exercise the brain is through brainwave entrainment. Isochronic tones are computer generated tones that are pulsed at specific frequencies to achieve desired effects such as productivity or relaxation. Although brainwave entrainment is not a new practice -- binaural beats have been used in brain training since the mid-1800's -- the use of computer generated isochronic tones has become more popular lately and are also proving to be more effective in helping people improve their memory and intelligence. Unfortunately when most people stop formal schooling, either by achieving a degree or choosing to drop out, the study habits and brain training that was part of their daily schedule also ends. The memorization and critical thinking that helped get us through school shouldn't have to stop just because a specific goal has been reached. In fact, if you don't keep up with brain exercises your mind will become lazy and won't function in the as sharply as it used to. The fact is, most people will never learn what it REALLY feels like to have their brains operating at a high capacity. They'll haphazardly try a few things, wonder why nothing is working, then go back to their mundane existence. But YOU can be different! You can use Genius Brain Power to empower your brain so that you come alive with more energy, learn quicker, think more creatively, focus on your work like never before and drastically reduce stress with amazingly deep states of relaxation and meditation. click here: http://brain-revitalizer.info-pro.co

Watch that video of Huge Foot blister Freezing With Liquid Nitrogen
Comment Avoir Un Ventre Plat, Rajeuni, Rajeunir De 10 Ans En 3 Mois, Bruleur De Graisse Musculation --- http://rajeunir-de-10-ans.info-pro.co --- 5 Raisons pourquoi le Cardio Long-Lent n’est PAS bon. En passant à travers les e-mails de clients au cours des derniers jours, j'ai remarqué que beaucoup de gens font encore du cardio longue durée, à faible intensité, beurk! Voici l'affaire: si vous cherchez à obtenir un bénéfice maximal du temps que vous mettez dans vos séances d'entraînement, le cardio de longue durée à faible intensité n'est pas la voie à suivre, et pour de nombreuses raisons. Voici mon top 5: 1. Les calories brûlées minimales: 45 minutes sur le tapis roulant peuvent brûler un énorme 300 calories si vous êtes chanceux, l'équivalent de 50 grammes de graisse. En vous exerçant dix heures par semaine et vous pourriez perdre un demi-kilo! Ce qui m'amène à mon prochain point: 2. Beaucoup trop de temps consacré: Je ne sais pas pour vous, mais je n'ai pas des heures et des heures de mon temps à mettre dans l’entraînement chaque semaine. En fait, je n’ai le temps pour faire que quelques heures d'exercice par semaine, et vous savez quoi? C'est tout ce dont vous avez besoin. En fait, la recherche a montré que plus de 90 minutes par semaine peuvent être nuisibles! (Plus d'infos ici) http://rajeunir-de-10-ans.info-pro.co Au-delà de cela, le cardio à longue durée et faible intensité est: 3. Ennuyeux que diable: Assis sur un vélo d'exercice à regarder le mur en face de moi pendant 45-60 minutes? Non merci. Mais peut-être pire encore est le fait que le cardio de longue durée et à faible intensité ne fournit: Ces 5 étapes Révèlent Les Choses Que Vous Devez ABSOLUMENT ÉVITER Si Vous Voulez Ralentir Le Processus De Vieillissement, Récupérer Votre Santé Et Atteindre Un Corps Idéal. Cliquez Ici: http://rajeunir-de-10-ans.info-pro.co
