- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos


Discover how hemodialysis works and the different options available for this dialysis treatment.
Related articles on DaVita.com:
What Is Hemodialysis? (http://www.davita.com/treatmen....t-options/hemodialys
How Does a Dialysis Machine Work? (http://www.davita.com/treatmen....t-options/hemodialys



Joe Ingles suffered a very bad looking injury on Sunday night in the NBA. In this video we'll review what happened and discuss the possibilities.
NBA and Basketball Videos:
https://youtube.com/playlist?l....ist=PLrdpldKEF234R2w
MY MUSIC:
Epidemic Sound - Sign up with this link for a FREE 30 day trial!
https://www.epidemicsound.com/referral/2m1bb5/
Follow Me on Twitter!
https://twitter.com/briansuttererMD
I'm a doctor and a sports fan and this channel is dedicated to exploring the unique medical side of the world of sports, including NBA, MLB, NFL, UFC, and many more! Breaking down the biggest what ifs, historical injuries and stories, and making learning about medicine fun and relevant for all sports fans!
Anatomy images: https://www.biodigital.com
DISCLAIMER: Content not intended to be taken as medical advice. Opinions are my own and do not represent those of my employer. I have not personally treated or evaluated the individual(s) discussed in this video. Content used with educational and transformative intent within Fair Use Guidelines
Content owned and produced by Brian Sutterer LLC 2022
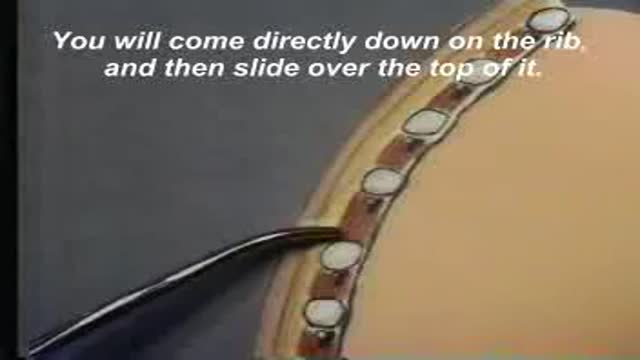
A video showing the insertion of chest tube

A video shows how to examine the hearing sensation
A video from Loyola medical school, Chicago showing the cardiovascular medical and clinical medical examination

Vertical Mattress Pattern Suture

Restoring Chipped Teeth

Esthetic Dentistry Today

Clonus is tested for in the ankles by rapidly dorsiflexing the relaxed ankle joint.

Intravitreal triamsinolon asetat injection following phacoemulsification

Foreign body bronchus removal

The Smallest Ultrasound device in the world

A video discussing the importance of following up the blood pressure for diabetic patients and the serious complications that they can avoid by this very simple measure.

The video will shed light on left upper lobe collapse
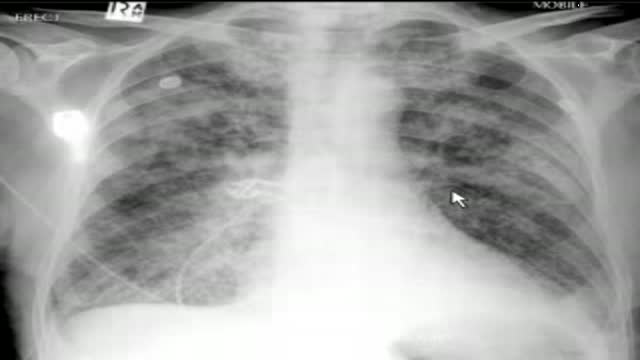
The video will describe pulmonary edema. Please see disclaimer on my website. www.academyofprofessionals.com

Laparoscopic Assisted Right Hemicolectomy
