- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
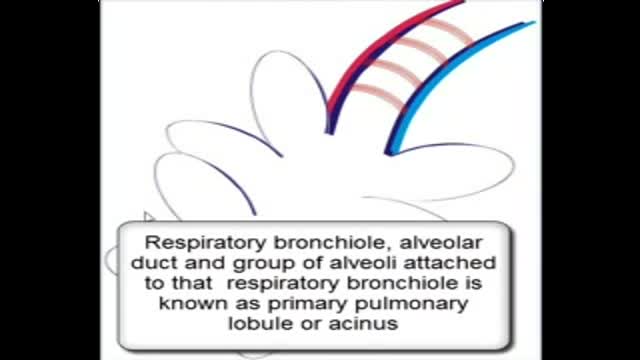
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Endoscopic Brain Surgery, third Ventriculostomy

Busa 08 í fs

NTI Tension Suppression System
Importance of Regular Dental Exams
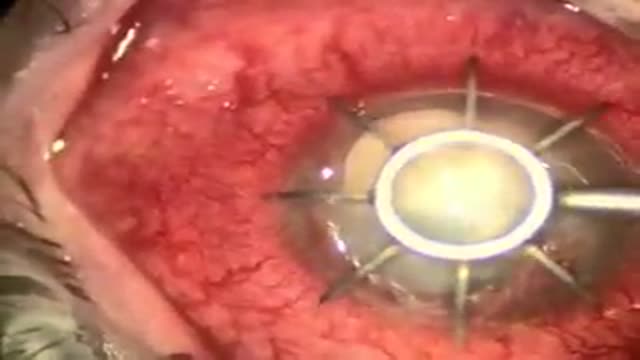
Cornea Transplant

Mesenteric artery illuminated with luciferase

Abdomen Waist Liposuction for Weight Loss

Rhinoplasty Surgery Video
This involves inserting a tube through the nasal passage, into the stomach
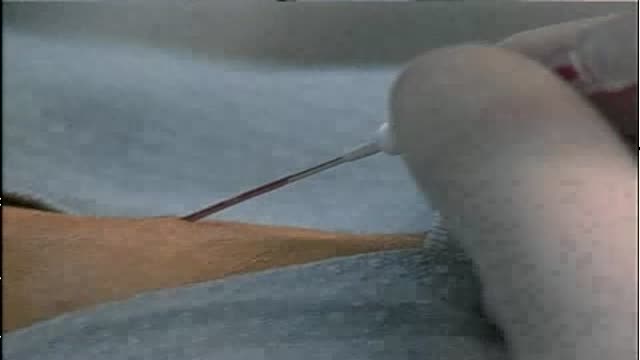
Radial Artery Catheterization

Swine Flu Avoid

The video will describe anatomy of thorax as seen on a chest lateral view.

A plastic surgery video showing Turbinal Reduction and Turbinoplasy of the nose
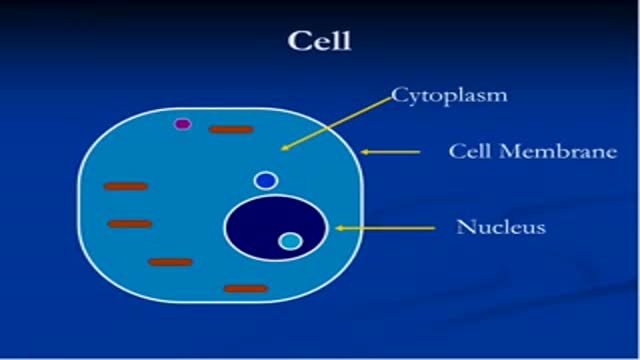
The third video about cell

DMC Neurosurgeon performs delicate brain surgery to remove a tumor pressing on a pateint's optic nerve. ~ Detroit Medical Center

Laparoscopic Repair of Rupture Urinary Bladder

Video of Cholecystectomy with common bile duct Exploration
As above. Please see disclaimer on my website. www.academyofprofessionals.com

The gallery of creative pharmaceutical advertisements
Eye Lid Plastic Surgery in Egypt video
