- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
http://tinnitus-solution.info-pro.co --- Ear Infection, Loud Ringing In Ears, Tinnitus Suicide, Ear Is Ringing, Tinnitus One Ear, Tinnitus. Do you suddenly get up in the middle of the night hearing strange noises? Yes it can definitely be frightening, more so when you cannot find the source. Now consider for a moment that these sounds are coming from within you. Most people would be stunned to know that. Many of us do not even know that our internal organs can make sounds. Let us try to see whether you actually heard these noises or not, and if you did, where did they come from. Now before anything, let us get this straight - yes, you actually heard those noises. No, they are not a result of a creative mind that imagined things in slumber. But having said that, it is also true that there is indeed no source of the sounds you heard. So what is it? Confused? This is a classic case of tinnitus. What is tinnitus? What you experienced last night (or did you just get up from sleep and switch on the computer) is a classic case of tinnitus. This is a medical condition wherein a person hears all kinds of strange clicking, ringing, buzzing, whistling or hissing sounds within the ear. What's so worrisome about this condition for a lot of people is that, there's actually no physical source of these sounds. What makes it even worse is that, no one else seems to hear them. Frankly, these people cannot be really blamed. Naturally, if you cannot see where the sound is coming from, and if you keep hearing it, you are bound to get worried. In tinnitus, the sounds a person hears are actually perceptions. Since there's no actual source, they are often referred to as "phantom noises". Will it help you if you knew that about 8% of all people in the US suffer from tinnitus? Perhaps not, but at least now you know that you are not alone who hears these strange noises. Cure tinnitus. this simple, but effective system to erasing Tinnitus out of your life for good has now helped cure over 105,302 people of all the frustrating ringing, hissing, buzzing. Even if you’ve tried every single tinnitus treatment or remedy under the sun. 100% natural tinnitus cure click here: http://tinnitus-solution.info-pro.co
Candidiase Tratamento, Remédio Para Unhas Com Fungos, Fungos Na Pele Como Tratar, Candidíase. http://candidiase-cura.plus101.com/ A intensa existência de substâncias químicas prejudiciais e metais tóxicos em nosso ambiente, nos medicamentos que tomamos, nos alimentos que comemos e até mesmo nos recheios dentários, cria um grande desafio para o nosso corpo se livrar efetivamente dessas toxinas resultando em uma ciclo vicioso que se manifesta em uma variedade de sintomas e problemas de saúde, entre eles é o crescimento excessivo de candida albicans que faz com que os sintomas da infecção por fungos aparecem. A acumulação de metais químicos e tóxicos no interior do corpo também pode levar a desequilíbrios hormonais, alterações genéticas, falhas no sistema imunológico, baixa eliminação, processo de cicatrização mais lenta, problemas de pele, alergias e danos no nervo e no cérebro. A presença de metais pesados ??no corpo (led, prata, mercúrio) proveniente de alimentos, o ar que respiramos, remédios e recheios dentários (contém 50% de amálgama), criam um ambiente ácido e anaeróbio (falta oxigênio) que incentiva a candida sobrecrescimento de fermento. Quando há sobrecarga de metal tóxico no intestino, o revestimento intestinal produz muco extra para impedir que os metais sejam absorvidos na corrente sanguínea. O problema é que esse muco cria um ambiente, que não possui oxigênio, incentivando bactérias e fungos, como organismos como o fermento Candida, a ficarem fora de controle. Além disso, a candida se liga a metais pesados ??(mesmo em seus enchimentos de amálgama) e cresce porque o corpo realiza uma tentativa desesperada de se proteger contra o envenenamento por metais pesados. Uma desintoxicação de metal profundo combinada com a remoção gradual do enchimento dentário de amalgama e substituindo-os por enchimentos brancos mais seguros é uma das etapas mais importantes e fundamentais na luta contra a infecção por levedura de Candida e restabelecendo o equilíbrio do corpo. O Único sistema holístico existente que vai lhe ensinar como curar Permanentemente sua Infecção fúngica, reequilibrar o seu corpo e conseguir a liberdade DURADOURA da Infecção do tipo candidíase! http://candidiase-cura.plus101.com/

Come Rimanere Incinta Subito, Probabilità Di Rimanere Incinta A 40 Anni, Primi Sintomi Gravidanza---- http://come-rimanere-incinta.info-pro.co --- Esperta in Medicina Cinese, Specializzata in Trattamenti per la Salute e in Nutrizione, Consulente per la Salute, Dopo Aver Provato in Prima Persona l'Infertilità e Averla Sconfitta ti Insegna Come: Rimanere Incinta in Modo Rapido e del Tutto Naturale in Soli 2 Mesi Dare alla Luce Bambini Sani e Forti Invertire il Problema dell'Infertilità, sia Maschile che Femminile Migliorare la Qualità della Tua Vita...Drasticamente! Scopri Come Ha Vinto la Sua Infertilità e Ha Insegnato a Migliaia di Donne in Tutto il Mondo Come Eliminare Tutti i Problemi dell'Infertilità e Come Rimanere Incinta in Modo Rapido e, Soprattutto, del Tutto Naturale Blog: http://bit.ly/2F3k8xR Se Stai Lottando con Tutte le Tue Forze per Rimanere Incinta e Nonostante Tutto Ancora Non Hai Ottenuto Risultati, Questa Sarà la Lettera Più Importante che Potrai Mai Leggere... Clicca sul link http://come-rimanere-incinta.info-pro.co

Watch that video of Unbelievable Mutations and Medical Conditions
Dieta Alcalina Recetas, Listado De Alimentos Alcalinos, Que Es El Agua Alcalina, Menu Para Adelgazar-- http://dieta-alcalina-alimentos.good-info.co -- Entendiendo los Efectos del nivel de pH en el cuerpo El nivel de pH en el cuerpo tiene la habilidad de afectar cada célula del cuerpo. Cuando la sangre tiene un pH alcalino en vez de un pH ácido, ocurre un efecto positivo en cada función corporal del sistema. El cerebro, el sistema circulatorio, los nervios, los músculos, el sistema respiratorio, el sistema digestivo y reproductivo se pueden beneficiar de un nivel adecuado de pH. Por otro lado, cuando el pH del cuerpo es muy ácido, es susceptible a muchas enfermedades y problemas. Ganancia de peso, enfermedades del corazón, envejecimiento prematuro, fatiga, problemas nerviosos, alergias, enfermedades musculares y cáncer son las más probables a ocurrir cuando el pH del cuerpo no está al nivel óptimo. Ya que todos estos problemas son más probables a ocurrir cuando el pH del cuerpo está muy ácido, tiene sentido consumir una dieta rica en alimentos alcalinos. El objetivo principal es usualmente comer aproximadamente entre 75-80% de alimentos alcalinos junto con solamente entre 20-25% de alimentos ácidos. Si se mantiene este nivel en la dieta, el resultado final es un nivel de pH bajo en el cuerpo, el que se requiere para una salud óptima. Descubre como la dieta alcalina funciona & por qué los alimentos alcalinos son altamente recomendados para tu salud. Haz clic aquí http://dieta-alcalina-alimentos.good-info.co
Polio virus

Blepharoplasty

Cerebellar functions of the upper limbs from the USMLE collection

Child Unresponsive Airway Obstruction
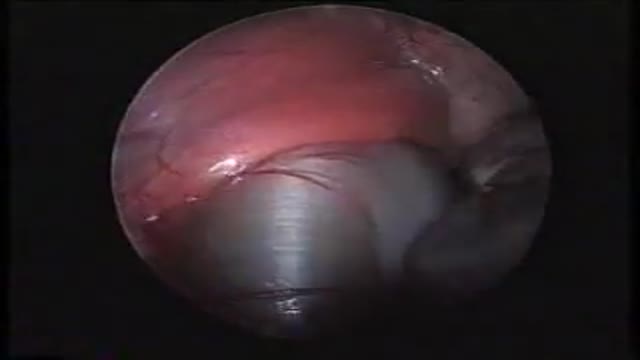
A laparoscopic view of the diaphragmatic hernia
Loyola oral Presentation for Rounds Part 1
Loyola oral Presentation for Rounds video

Tie

Subcutaneous Pattern Suture
MEdRC is a medical elearning company in India.
Aortic Valve-Sparing Operation in a Patient with Aortic Root Aneurysm using a new Prosthesis for Anatomical Reconstruction of the Sinuses of Valsalva

Repair techniques for various types of asymmetric pectus excavatum are illustrated. Morphology-tailored bar shaping and selecting the hinge points are key elements of the technique. Repair of two cases on an eccentric type and unbalanced type according to "Park Classification" was demonstrated.
Trabeculectomy with mitomycin-C for complex glaucoma. video

Aortic Valve Replacement Animation

How bunions appear
