- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Signs and symptoms of chronic kidney disease develop over time if kidney damage progresses slowly. Signs and symptoms of kidney disease may include: Nausea Vomiting Loss of appetite Fatigue and weakness Sleep problems Changes in how much you urinate Decreased mental sharpness Muscle twitches and cramps Swelling of feet and ankles Persistent itching Chest pain, if fluid builds up around the lining of the heart Shortness of breath, if fluid builds up in the lungs High blood pressure (hypertension) that's difficult to control Signs and symptoms of kidney disease are often nonspecific, meaning they can also be caused by other illnesses. Because your kidneys are highly adaptable and able to compensate for lost function, signs and symptoms may not appear until irreversible damage has occurred.
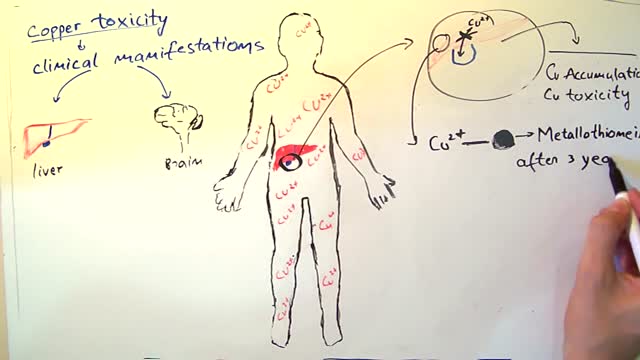
Wilson's disease is a rare inherited disorder that causes too much copper to accumulate in your liver, brain and other vital organs. Symptoms typically begin between the ages of 12 and 23. Copper plays a key role in the development of healthy nerves, bones, collagen and the skin pigment melanin. Normally, copper is absorbed from your food, and any excess is excreted through bile — a substance produced in your liver. But in people with Wilson's disease, copper isn't eliminated properly and instead accumulates, possibly to a life-threatening level. When diagnosed early, Wilson's disease is treatable, and many people with the disorder live normal lives.
Examination of the Eyes and Vision

Alzheimer's worsens over time. Alzheimer's is a progressive disease, where dementia symptoms gradually worsen over a number of years. In its early stages, memory loss is mild, but with late-stage Alzheimer's, individuals lose the ability to carry on a conversation and respond to their environment. Alzheimer's is the sixth leading cause of death in the United States. Those with Alzheimer's live an average of eight years after their symptoms become noticeable to others, but survival can range from four to 20 years, depending on age and other health conditions. Alzheimer's has no current cure, but treatments for symptoms are available and research continues. Although current Alzheimer's treatments cannot stop Alzheimer's from progressing, they can temporarily slow the worsening of dementia symptoms and improve quality of life for those with Alzheimer's and their caregivers. Today, there is a worldwide effort under way to find better ways to treat the disease, delay its onset, and prevent it from developing. Alzheimer's has no current cure, but treatments for symptoms are available and research continues. Although current Alzheimer's treatments cannot stop Alzheimer's from progressing, they can temporarily slow the worsening of dementia symptoms and improve quality of life for those with Alzheimer's and their caregivers. Today, there is a worldwide effort under way to find better ways to treat the disease, delay its onset, and prevent it from developing.

The DASH diet is a lifelong approach to healthy eating that's designed to help treat or prevent high blood pressure (hypertension). The DASH diet encourages you to reduce the sodium in your diet and eat a variety of foods rich in nutrients that help lower blood pressure, such as potassium, calcium and magnesium.
Shoulder pain and exercises Milwaukee WI

As a result, the amount of glucose in the blood increases while the cells are starved of energy. Over time, high blood glucose levels damage nerves and blood vessels, leading to complications such as heart disease and stroke, the leading causes of death among people with diabetes.

Warfarin is an anticoagulant medication - it is used to slow down the blood-clotting process. Anticoagulants are used to prevent blood clots which may cause vein blockages, heart attack and stroke. Warfarin is known under the brand names Warfant, Jantoven, Coumadin, Lawarin, Marevan, and Waran.
People with serious comprehension difficulties have what is called Wernicke’s aphasia and: Often say many words that don’t make sense. May fail to realize they are saying the wrong words; for instance, they might call a fork a “gleeble.” May string together a series of meaningless words that sound like a sentence but don’t make sense. Have challenges because our dictionary of words is shelved in a similar region of the left hemisphere, near the area used for understanding words.
Head Cyst watch to see more

Laryngeal Mask Airway in Medical Emergencies

Lewy body dementia, also known as dementia with Lewy bodies, is the second most common type of progressive dementia after Alzheimer's disease dementia. Protein deposits, called Lewy bodies, develop in nerve cells in the brain regions involved in thinking, memory and movement (motor control). Lewy body dementia causes a progressive decline in mental abilities. People with Lewy body dementia may experience visual hallucinations, and changes in alertness and attention. Other effects include Parkinson's disease-like symptoms such as rigid muscles, slow movement and tremors.
No Need For An Endoscopy With This Cancer-Detecting Sponge.

If you're sensitive do not watch this videoEmergent Tracheotomy!
Scientists are working on a pill that could replace exercise.

Gallbladder & Gallstone Removal Surgery
Home Remedies For Acid Reflux, Ginger For Acid Reflux, Heartburn After Gallbladder Removal --- http://heartburn-acid-reflux.info-pro.co --- Stop using Pepto Bismol until you read the following… There is BREAKING scientific news reporting that many of America’s most popular antacids – both the ones you buy at the drug store and the ones you need prescriptions for… Are linked to more than a dozen forms of potentially DEADLY cancers. Click this link now to get the full story and see if you’re at risk. You’ll find out about a “just discovered” alternative to antacids…. Something that can permanently cure even the worst cases of acid reflux in as little few days, and that doesn’t require any pills or medications. Click Here: http://heartburn-acid-reflux.info-pro.co

Is Shingles Contagious, What Are Shingles, Herpes Zoster Pictures, Shingles Home Remedies --- http://shingles-cure.good-info.co/ --- If You Are A Newcomer To This Disease, I Hate To Be The Bringer Of Bad News But You Should Know That The List Of Potential Symptoms Is Depressingly Long. These Include The Following: A General Feeling Of Muscle Pain To Begin With, Almost Like Flu A Tingling, Burning Type Sensation In A Specific Area Of The Skin Fever And Headache And Sometimes A Swelling Of The Lymph Nodes A Band Of Spots And Then A Rash At A Specific Part Of Your Body – Very Often The Head Or The Side Of The Trunk Infection Over The Site Of The Rash – Leaving It Prone To Additional Tissue Damage From Bacteria Postherpetic neuralgia leading to chronic nerve pain Ulceration Of The Eye – In Those Cases Where The Shingles Rash Occurs In The Area Of The Eye – Known As Zoster Ophthalmicus. Stress And Depression – Particularly Where The Illness Lingers On For A Long Period Everyone Is Different And Not Everyone Will Experience All Of Those Symptoms. However Even The Most Mild Case Of Shingles Can Be Extremely Debilitating – Something Of Which I Am All Too Aware. Tired Of Fighting A Never Ending Battle Against Shingles? Sick Of Being Told That There´s Nothing You Can Do To Speed Up Recovery? Wherever You Are In Your Fight Against Shingles, I Can Help In this presentation, shows you some unique and rare methods to get rid of shingles naturally in as little as 14 days! This is based on proven techniques used by shingles sufferers without the use of pills and other medication. Get Rid of Shingles will also boost your energy and health dramatically and improve the quality of your life. IMPORTANT NOTE: I can't leave this video up for long, so be sure to watch it from beginning to end while it's still here. REMEMBER: Watch the whole video, as the ending will pleasantly surprise you. click here: http://shingles-cure.good-info.co/
Watch that video of the Worst Brain & Liver Cysts Removal\
Como Aumentar La Libido, Aumentar Niveles De Testosterona, Como Aumentar El Deseo Masculino ---- http://aumentar-testosterona.good-info.co/ --- ¿Se puede tener una erección con bajos niveles de testosterona? Mi libido está quedando atrás y estoy teniendo dificultades para conseguir una erección, así que estoy tratando de averiguar qué está pasando aquí. La disfunción eréctil rara vez es causada sólo por la deficiencia de testosterona. Por lo general es un grupo de cosas que funcionan en concierto juntos, que se alimentan entre sí, que conducen a la incapacidad del hombre para lograr una erección. La aterosclerosis (estrechamiento y endurecimiento de las arterias) es uno de los mayores impulsores de la disfunción eréctil, pero estas arterias dañadas no aparecen de la nada. Otras cosas tienen que estar sucediendo en el cuerpo para que ésta aterosclerosis pase, y como estamos a punto de ver, estas otras cosas contribuyen al problema también. Así que vamos a repasar esta lista… Nivel de azúcar alto – baja testosterona y disfunción eréctil La azúcar elevada en la sangre es un arma de doble filo, porque los hombres que sufren de esta condición son mucho más propensos a ser afectados por la disfunción eréctil y la testosterona baja. Una Investigación de John Hopkins encontró que las ratas diabéticas presentaron una respuesta eréctil 30% inferior, sus erecciones fueron como máximo 40% más pequeñas y las erecciones tomaron 70% más tiempo para lograrse en comparación con los controles que no eran diabéticos. Otros estudios han confirmado que los hombres con diabetes tipo 2 son dos veces más propensos a sufrir de disfunción eréctil, y la condición les golpeará una década antes, en comparación con los hombres sin tipo 2. Este vínculo es tan fuerte porque el azúcar en la sangre hace un daño directo a las arterias cuando se tiene demasiado de él, y las arterias en el pene suelen ser afectados en primer lugar, porque son muy pequeñas y estrechas. Por lo tanto, tiene todo el sentido que éstas pueden dañarse primero. El ejercicio que baja la testosterona haga click aqui http://aumentar-testosterona.good-info.co/
