- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
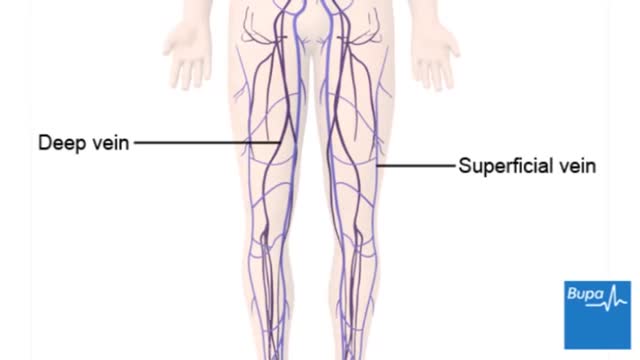
Deep vein thrombosis (DVT) occurs when a blood clot (thrombus) forms in one or more of the deep veins in your body, usually in your legs. Deep vein thrombosis can cause leg pain or swelling, but may occur without any symptoms. Deep vein thrombosis can develop if you have certain medical conditions that affect how your blood clots. Deep vein thrombosis can also happen if you don't move for a long time, such as after surgery, following an accident, or when you are confined to a hospital or nursing home bed.

Watch that video to know The 8 Types Of Female Genital Discharge

Watch that Stuck Sex Toy Removal Surgery
These are a few common types of benign bone tumors: Osteochondroma is the most common benign bone tumor. ... Giant cell tumor is a benign tumor, typically affecting the leg (malignant types of this tumor are uncommon). Osteoid osteoma is a bone tumor, often occurring in long bones, that occurs commonly in the early 20s.
Recently a group of affected females from Cameroon has started raising the voices against an old cultural "Female Abuse" tradition which is "Breast Ironing". The point of this tradition is to inhibit the growth of the female breast so that they will avoid getting raped.

jbkbkbkbkj

Tears Of Abortion - Story of an aborted baby,
Here's how female-to-male gender reassignment surgery works.
The Epley maneuver is a series of movements, normally carried out on a person by a doctor, to relieve the symptoms of BPPV. Research has found it to be an easy, safe, and effective treatment for the condition in both the long- and short-term. The Epley maneuver is sometimes called the particle repositioning maneuver or the canalith repositioning maneuver. These names are used because the maneuver involves a series of movements that help to reposition crystals in a person's ear that may cause feelings of dizziness. Repositioning the crystals helps to relieve the person's dizziness and nausea.

Spigelian Hernia on Ultrasound

Incision and Drainage of a Huge Gluteal Abscess
USMLE Step 2 CS - BPH - This is just preview video. To get full access please visit our website : www.usmletutoring.com
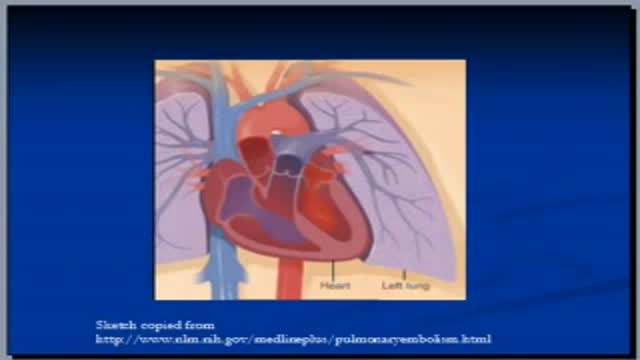
The video is second of three to discuss the topic of pulmonary embolism. Please see website for disclaimer.
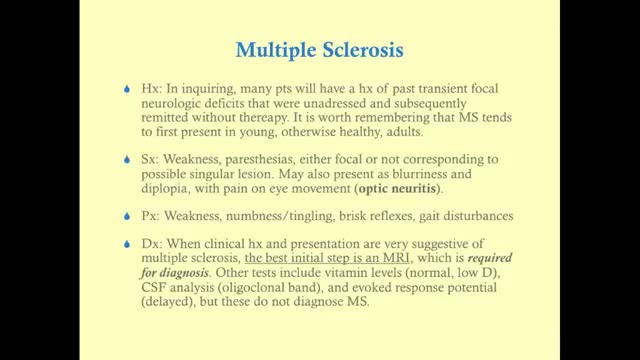
Multiple sclerosis (MS) affects the brain and spinal cord. Early MS symptoms include weakness, tingling, numbness, and blurred vision. Other signs are muscle stiffness, thinking problems, and urinary problems. Treatment can relieve MS symptoms and delay disease progression.

Plantar warts are hard, grainy growths that usually appear on the heels or balls of your feet, areas that feel the most pressure. This pressure also may cause plantar warts to grow inward beneath a hard, thick layer of skin (callus). Plantar warts are caused by the human papillomavirus (HPV). The virus enters your body through tiny cuts, breaks or other weak spots on the bottom of your feet. Most plantar warts aren't a serious health concern and may not require treatment. But plantar warts can cause discomfort or pain. If self-care treatments for plantar warts don't work, you may want to see your doctor to have them removed.

You may have heard that some positions, such as your partner on top (missionary position), are better than others for getting pregnant. In fact, there's no evidence to back these theories up. Experts just haven't done the research yet. What experts have done, though, is use scanning to show what's going on inside when you're doing the deed. The research looked at two positions: the missionary position and doggy style. (Doggy style being when you're on all fours, and your partner enters you from behind). Common sense tells us that these positions allow for deep penetration. This means that they're more likely to place sperm right next to your cervix (the opening of your uterus). The scans confirm that the tip of the penis reaches the areas between the cervix and vaginal walls in both of these positions. The missionary position allows the penis to reach the area at the front of the cervix. The rear entry position reaches the area at back of the cervix. It's amazing what some experts spend their time doing, isn't it! Other positions, such as standing up, or woman on top, may be just as good for getting sperm right next to the cervix. We just don't know yet. http://www.babycentre.co.uk/sex-for-getting-pregnant#ixzz4XKnPLbxL

The fetal circulation is the circulatory system of a human fetus, often encompassing the entire fetoplacental circulation that also includes the umbilical cord and the blood vessels within the placenta that carry fetal blood.
The fetal circulation works differently from that of born humans, mainly because the lungs are not in use: the fetus obtains oxygen and nutrients from the mother through the placenta and the umbilical cord.
DOING LESS BUT BRAINY DESCRIBES A NEW GENERATION OF IMMEDIATE ZIRCONIA IMPLANTS ANATOMICAL AND CUSTOM-MADE. YOUR DENTAL ROOT IS MILLED IN ZIRCONIA AND IN 20 SECONDS SEATED, NO DRILLING, NO AUGMENTATION, NO MEMBRANES, FLAPLESS, NO 3D PLANNING, NO CAD/CAM SPLINTS OR GUIDED SURGERY REQUIRED! EASY AND CONSEQUENTIAL SYSTEM. NO MORE INCONGRUOUS AND UGLY SILVER-COLORED TITANIUM IMPLANTS IN TIME CONSUMING, PAINFUL AND COSTLY PROCEDURES. IT`S HIGH TIME TO RESPECT THE ANATOMY NOT ALTER IT BY DRILLING AND AUGMENTATION. BIOIMPLANT

Excision of Pilonidal Cyst. Open method.

Diabetic retinopathy involves changes to retinal blood vessels that can cause them to bleed or leak fluid, distorting vision. Diabetic retinopathy is the most common cause of vision loss among people with diabetes and a leading cause of blindness among working-age adults.
