- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
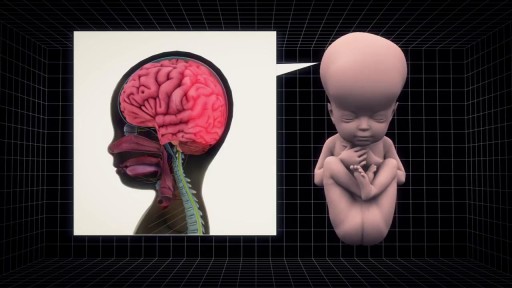
Hydrocephalus can be fatal if left untreated. The damage to the brain can cause headaches, vomiting, blurred vision, cognitive problems, and walking difficulties. The term water on the brain is incorrect, because the brain is surrounded by CSF (cerebrospinal fluid), and not water.Oct 8, 2015

IMPLANT POCKETS - an educational animation explaining the different implant pockets

Subscribe and 🔔 to the BBC 👉 https://bit.ly/BBCYouTubeSub
Watch the BBC first on iPlayer 👉 https://bbc.in/iPlayer-Home http://www.bbc.co.uk/human Richard Edwards undergoes a double hand transplant in which his hands are amputated and replaced with hands from a donor. This is the first time this has been done. Three months later the new hands are already changing his life.
#bbc
All our TV channels and S4C are available to watch live through BBC iPlayer, although some programmes may not be available to stream online due to rights. If you would like to read more on what types of programmes are available to watch live, check the 'Are all programmes that are broadcast available on BBC iPlayer?' FAQ 👉 https://bbc.in/2m8ks6v.
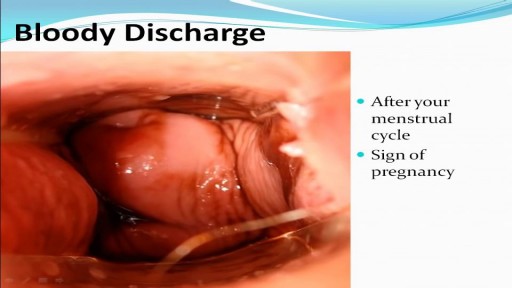
Watch that video to know the Types of Female Genital discharge

watch that Enema Insertion Medical Procedure

Watch that video to know The 8 Types Of Female Genital Discharge

Watch that video to know the Serious Side Effects of STEROIDS on Human Body
To identify an UTI, keep an eye out for the following symptoms: A burning feeling when you urinate. A frequent or intense urge to urinate, even though little comes out when you do. Pain or pressure in your back or lower abdomen. Cloudy, dark, bloody, or strange-smelling urine. Feeling tired or shaky.

In this video, Professor Dan Reinstein performs a bilateral LASIK procedure filmed in real-time to demonstrate the full 8 and-a-half minute procedure from multiple angles. The superior design and experience of the Carl Zeiss Meditec Visumax femtosecond Laser for flap creation is seen, where the patient is only in contact with the device for about 30 seconds with extremely low contract force such that the patient feels effectively nothing, there are no red splodges (subconjunctival haemorages) left behind. From the surgeons' standpoint there is no device that is easier to use or faster for LASIK flap creation. The Carl Zeiss Meditec MEL80 excimer laser portion of the procedure is seamlessly integrated and incorporates all the features that make clinical outcomes so reproducible including the unique cone-for-controlled-atmosphere (CCA) and high efficiency, high sensitivity calibration test which can be performed for each individual patient to compensate for minor changes in energy that occur with excimer laser devices during the course of a day.
For reference to the clinical outcomes for LASIK with the MEL80 in presbyopia using PRESBYOND Laser Blended Vision see:
Reading glasses presbyopia (ageing eyes) only:
LASIK for presbyopia correction in emmetropic patients using aspheric ablation profiles and a micro-monovision protocol with the Carl Zeiss Meditec MEL 80 and VisuMax.
J Refract Surg. 2012 Aug;28(8):531-41. Reinstein DZ, Carp GI, Archer TJ, Gobbe M.
http://www.ncbi.nlm.nih.gov/pubmed/22869232
Short sighted, astigmatism and presbyopia (ageing eyes)
LASIK for Myopic Astigmatism and Presbyopia Using Non-Linear Aspheric Micro-Monovision with the Carl Zeiss Meditec MEL 80 Platform.
J Refract Surg. 2011 Jan;27(1):23-37. Epub 2010 Mar 1.
Reinstein DZ, Archer TJ, Gobbe M.
http://www.ncbi.nlm.nih.gov/pubmed/20205360
Long-sighted, astigmatism and presbyopia (ageing eyes)
LASIK for hyperopic astigmatism and presbyopia using micro-monovision with the Carl Zeiss Meditec MEL80 platform.
J Refract Surg. 2009 Jan;25(1):37-58. Reinstein DZ, Couch DG, Archer TJ.
http://www.ncbi.nlm.nih.gov/pubmed/19244952
For more information about laser eye surgery and PRESBYOND Laser Blended Vision, please contact the London Vision Clinic on 020 7224 1005.

A Pfannenstiel incision /ˈfɑːnᵻnʃtiːl/ is a type of abdominal surgical incision that allows access to the abdomen. It is used for gynecologic and orthopedics surgeries, and it is the most common method for performing Caesarian sections today.

The video is about the evolution of the anatomic UCLA laparoscopic technique over 1325 cases and demonstrates the key steps of our operation to improve patient safety and outcomes.
Learn more at http://urology.ucla.edu
Endoscopy of Mammary Ducts with Micro-Endoscope called Mammary Ductoscopy. Indication:- Nipple Discharge. In this case Papilloma seen quite clearly. Biopsy can also be possible with Ductoscopy. Mammary Ductoscopy is very useful for diagnosis of Breast Cancer in early stage.

Vaginoplasty is a surgical procedure designed to rejuvenate and tighten a woman’s vagina, by removing excess lining and repairing the surrounding soft tissues. It is designed to decrease the diameter of the vagina, resulting in increased friction during intercourse to make the experience more pleasurable for both partners.

Testis operation

Best and 100% Successful Hymen Repair Surgery in Delhi with Latest Ultrafine Hymen repair Technology. 100% successful , Secure and Private. for more information visit: http://www.olmeccosmeticsurgery.com/best-hymenoplasty-surgery-india-delhi/

This video: Patent ductus arteriosus (PDA) is a persistent opening between two major blood vessels leading from the heart. The opening, called the ductus arteriosus, is a normal part of a baby's circulatory system before birth that usually closes shortly after birth. If it remains open, however, it's called a patent ductus arteriosus. A small patent ductus arteriosus often doesn't cause problems and might never need treatment. However, a large patent ductus arteriosus left untreated can allow poorly oxygenated blood to flow in the wrong direction, weakening the heart muscle and causing heart failure and other complications. Treatment options for a patent ductus arteriosus include monitoring, medications and closure by cardiac catheterization or surgery.

Breast Augmentation Plastic Surgery Video

Originally broadcast November 21, 2014.
They advertise low, low prices. But does anyone actually pay that rate? Erica Johnson investigates.
More from CBC Marketplace, Canada's top consumer affairs show:
Watch episodes online at http://cbc.ca/marketplace
Like us on Facebook: http://facebook.com/cbcmarketplace
Talk to us on Twitter: http://twitter.com/cbcmarketplace
Follow our hosts @cbctom and @cbcerica
Loyola Respiratory System Exam Part 1 A video from Loyola Medical School, Chicago showing the medical and clinical examination of the respiratory system.

Watch that video of Bodybuilder's Colon Full of 10 lbs of Meat Worms Removal
