- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

nkylosing spondylitis (pronounced ank-kih-low-sing spon-dill-eye-tiss), or AS, is a form of arthritis that primarily affects the spine, although other joints can become involved. It causes inflammation of the spinal joints (vertebrae) that can lead to severe, chronic pain and discomfort

What to expect during the day of a pediatric surgery at Sutter Children's Center Sacramento.

Commentary:
0:24
He may not look like he’s in good condition but you can guesst that his somewhere in nirvana at this point
0:44
After the operation, this patient loses more than just color in his skin but apparently he loses his nipples as well
1:43
This sedated patient is equipped with his own hand-gun. No pun intended
2:17
His anesthesia dose came with the usual side effects of crazy talk with a dash of attitude and sarcasm
3:17
The only thing crazier than love is being sedated during an endometriosis surgery
4:36
This may come as a surprise to some but penguins don’t actually reside in Alaska. In case you didn’t know that well now you do
5:09
If the doctor advises you against something you can’t resist doing, how many of us would still listen to him?
6:35
When them meds start kicking in , it’s time to frame this experience as an excuse to divulge some of your secret fantasies
7:05
There’s a time and place dirty jokes but anesthesia told this guy any times the right time
7:24
Her 16 year old son talks about the last thing he remembers right after surgery and this is what he says
8:35
She’s definitely not in the mood at all. I wouldn’t wanna tick her off during this time if I were you
8:44
A feeling of relief after your operation may be followed by some emotional changes such as mood swings and over sensitivity
9:44
Even if you do say something you wouldn't normally say while you are under sedation, according to some doctors, “it's always kept within the operating room”
10:38
The beeping sounds of the medical equipments tip this patient over the edge. so she tries to drown out the noise with her own voice
11:08
Anyone who's received anesthesia can attest to feeling pretty loopy. Although many won't remember it's fairly common to say some wacky things after waking up
11:53
It's typical for people to feel sad or vulnerable after surgery. Kind of like how this girl is feeling right now
12:04
If she wasn’t under the influence in the hospital right now , it would be pretty hard to justify this type of behavior
12:17
Imagine working as an anesthesiologist. You might become numb to a lot of strange behaviors and everything unusual becomes the new norm for you
► Subscribe: https://bit.ly/3I4zXBT
Top Special Videos: https://bit.ly/3o64YOa
Acts Of Kindness: https://bit.ly/3E5FmXh
Try Not To Laugh Videos: https://bit.ly/3leRpdl
Social media:
► INSTAGRAM: https://www.instagram.com/topthings.tt/
► FACEBOOK: https://www.facebook.com/TopTh....ings-108385027422972
► TWITTER: https://twitter.com/TopThings10
► YOUTUBE: https://www.youtube.com/channe....l/UCArcrGQYzJhB_IfEl
#funnyvideos #anesthesia #anesthesiareactions
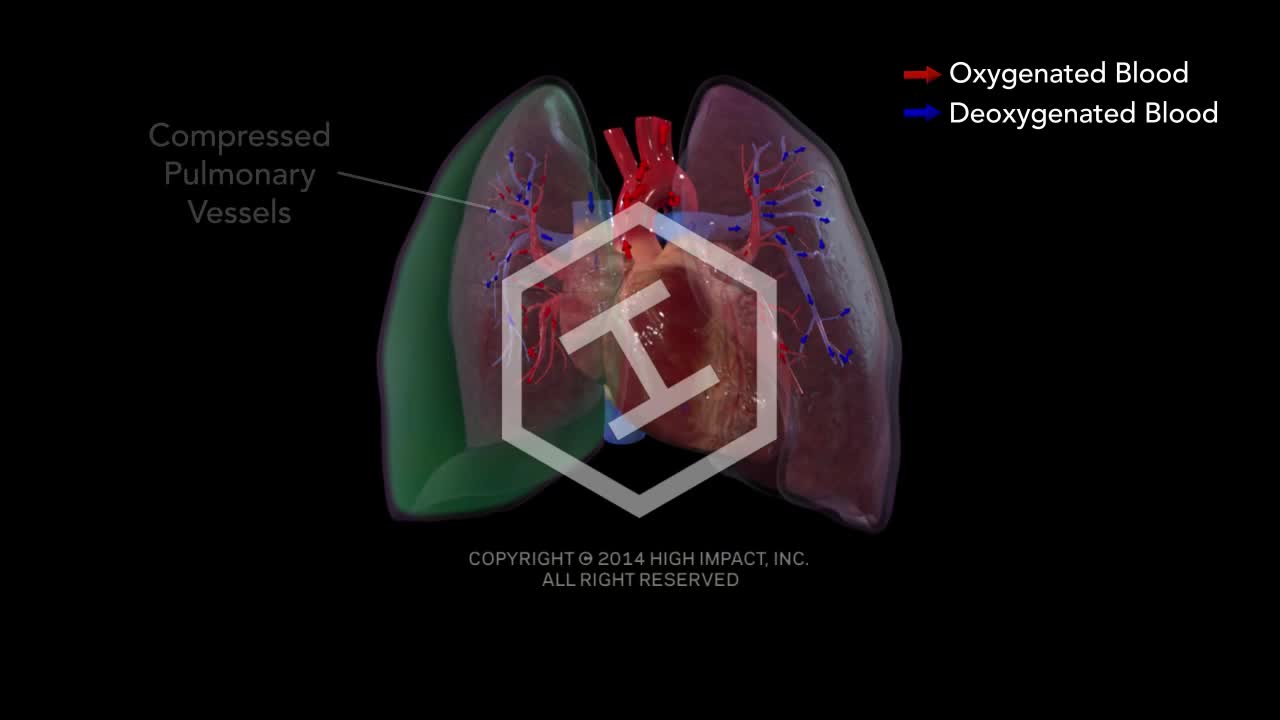
Tension pneumothorax develops when a lung or chest wall injury is such that it allows air into the pleural space but not out of it (a one-way valve). As a result, air accumulates and compresses the lung, eventually shifting the mediastinum, compressing the contralateral lung, and increasing intrathoracic pressure enough to decrease venous return to the heart, causing shock. These effects can develop rapidly, particularly in patients undergoing positive pressure ventilation.

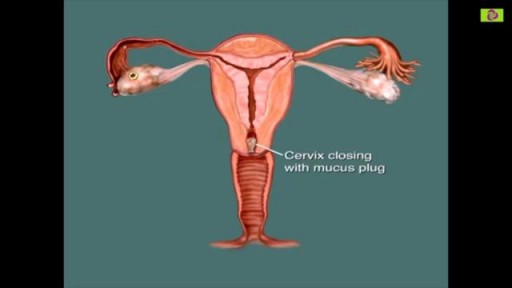
You are most fertile at the time of ovulation, (when an egg is released from your ovaries) which usually occurs 12-14 days before your next period starts. This is the time of the month when you are most likely to get pregnant. It is unlikely that you will get pregnant just after your period, although it can happen.

Alcoholic hepatitis is inflammation of the liver caused by drinking alcohol. Alcoholic hepatitis is most likely to occur in people who drink heavily over many years. However, the relationship between drinking and alcoholic hepatitis is complex. Not all heavy drinkers develop alcoholic hepatitis, and the disease can occur in people who drink only moderately. If you're diagnosed with alcoholic hepatitis, you must stop drinking alcohol. People who continue to drink alcohol face a high risk of serious liver damage and death.

During a standard abdominoplasty, Dr. Sanchez removes the excess skin of the lower abdomen. He repairs separated muscles, and pulls the skin down nice and tight. Lastly, a new hole is cut into the skin for the belly button. Let us know your questions!
To request a consultation with Dr. Sanchez, visit sanchezplasticsurgery.com and click Request a Consultation. Fill out the form and someone will get in touch with you to answer all your questions.

Be sure to have your teenager checked for hernias as they may be malevolent, Dr. Honaker gives us some insight as to why this is an important thing to have done.
A bone marrow biopsy removes a small amount of bone and a small amount of fluid and cells from inside the bone (bone marrow). A bone marrow aspiration removes only the marrow. These tests are often done to find the reason for many blood disorders and may be used to find out if cancer or infection has spread to the bone marrow. Bone marrow aspiration removes a small amount of bone marrow fluid and cells through a needle put into a bone. The bone marrow fluid and cells are checked for problems with any of the blood cells made in the bone marrow. Cells can be checked for chromosome problems. Cultures can also be done to look for infection. A bone marrow biopsy removes bone with the marrow inside to look at under a microscope. The aspiration (taking fluid) is usually done first, and then the biopsy.

For more videos, please visit:
http://surgicalfilmatlas.mssm.edu/

It used to be when a woman needed a hysterectomy she could expect full abdominal surgery with a long recovery time. Dr. Melissa Lee uses less invasive methods that can cut the patients downtime in half.
"We were trained in more laparoscopic and minimally invasive cases so of course that's what I'm more comfortable with doing right now."
She sees a new generation of patients opting for laparoscopic surgery.
"Laparoscopy is the use of small cameras with small incisions and instruments that are guided by the hand, and you're able to see directly into the abdomen without actually fully opening the abdomen," says Dr. Lee, an obstetrician-gynecologist with Lee Memorial Health System.
Nowadays, even a large mass or uterus can be removed using the slender tools.
"There are multiple different laparoscopic instruments that you can use. Whether they're blunt dissections or just dissectors that hold and retract back or actual scissors or cutting instruments, there are multiple different options," says Dr. Lee.
While a standard abdominal hysterectomy requires a four to eight inch incision, the laparoscope needs only a quarter to half inch. It's enough to make a big difference in terms of recovery.
"They're able to get up and move around faster. They're able to recover faster, their pain level and their need for pain medicine is much lower," says Dr. Lee.
The laparoscopic procedure also cuts down on scarring and more importantly, shortens the hospital stay. The trend now is home within 24 hours.
"Where the patient is done early in the morning, they're doing well they're tolerating oral intake they're able to getup and move around. And those patients a lot of times will feel comfortable to go home that same nigh after a major surgery," says Dr. Lee.
New studies show women who've had a laparoscopic hysterectomy viewed their quality of life as better than those who had an open abdominal procedure, making this a good option for the right patient.
View More Health Matters video segments at leememorial.org/healthmatters/
Lee Memorial Health System in Fort Myers, FL is the largest network of medical care facilities in Southwest Florida and is highly respected for its expertise, innovation and quality of care. For nearly a century, we've been providing our community with everything from primary care treatment to highly specialized care services and robotic assisted surgeries.
Visit leememorial.org
Abdominal Physical Examination Lecture

heart dissection / cardiac anatomy

Surgical procedure of Tonsillectomy and Adenoidectomy

Watch more clips of Dr. James Kelly - https://www.youtube.com/playli....st?list=PLe2Je5-cHxP And for more information about brain injury and PTSD, please visit us at https://www.brainline.org.
Watch more clips of Pat LaFontaine - https://www.youtube.com/playli....st?list=PL5F3273C3C8
© 2018 WETA All Rights Reserved
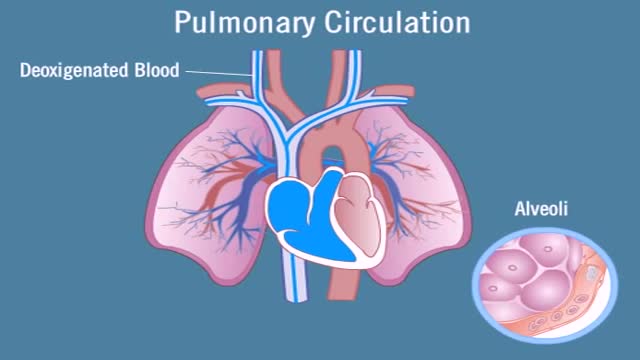
Pulmonary circulation is the portion of the cardiovascular system which carries deoxygenated blood away from the heart, to the lungs, and returns oxygenated (oxygen-rich) blood back to the heart. The function of pulmonary circulation is to exchange carbon dioxide for oxygen in the blood. It is the passage of blood from the heart to the capillaries of the lungs, where the gases are exchanged, and back to the heart to be pumped around the body.

How Liposuction Works in 15 seconds.
See how we illustrated this amazing technology by Alma Lasers.
Curious 🤔 about medical device 3D animation? ➜ http://www.arcreative-media.com

G-Shot (G-Spot Amplification)

A little venom is drawn into a syringe. ... The quick coagulation or blood clotting caused by the Russell's viper venom is of particular interest to scientists — there's a lot of research into how it might be used in medicine. But this effect is only present in healthy blood.
