- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

show your patients how to use an inhaler

Breast Augmentation Plastic Surgery Video

This video: Pancreatic cancer begins in the tissues of your pancreas — an organ in your abdomen that lies horizontally behind the lower part of your stomach. Your pancreas secretes enzymes that aid digestion and hormones that help regulate the metabolism of sugars. Pancreatic cancer often has a poor prognosis, even when diagnosed early. Pancreatic cancer typically spreads rapidly and is seldom detected in its early stages, which is a major reason why it's a leading cause of cancer death. Signs and symptoms may not appear until pancreatic cancer is quite advanced and complete surgical removal isn't possible.
The kidneys are a pair of organs located in the back of the abdomen. Each kidney is about 4 or 5 inches long -- about the size of a fist. The kidneys' function are to filter the blood. All the blood in our bodies passes through the kidneys several times a day. The kidneys remove wastes, control the body's fluid balance, and regulate the balance of electrolytes. As the kidneys filter blood, they create urine, which collects in the kidneys' pelvis -- funnel-shaped structures that drain down tubes called ureters to the bladder. Each kidney contains around a million units called nephrons, each of which is a microscopic filter for blood. It's possible to lose as much as 90% of kidney function without experiencing any symptoms or problems.

How to give Intramuscular (IM) injection


Vaginoplasty is a surgical procedure designed to rejuvenate and tighten a woman’s vagina, by removing excess lining and repairing the surrounding soft tissues. It is designed to decrease the diameter of the vagina, resulting in increased friction during intercourse to make the experience more pleasurable for both partners.

If you notice a patient beginning to fall, follow these steps to help lower them safely to floor. Always stay with the patient and call for additional help.
Download the CNA Mastery app: https://onelink.to/cnamastery
Download the My Mastery nursing app: https://mynursingmastery.com/get-started

Best and 100% Successful Hymen Repair Surgery in Delhi with Latest Ultrafine Hymen repair Technology. 100% successful , Secure and Private. for more information visit: http://www.olmeccosmeticsurgery.com/best-hymenoplasty-surgery-india-delhi/

A man's age matters. As men get older, the chances of conceiving and having a healthy child decline. Male fertility starts to decline after 40 when sperm quality decreases. This means it takes longer for their partners to conceive and when they do, there's an increased risk of miscarriage.

WORLD'S FIRST TRULY ANATOMIC MULTI-ROOTED ZIRCONIA DENTAL IMPLANT SOLUTION dentistry video

This video: Patent ductus arteriosus (PDA) is a persistent opening between two major blood vessels leading from the heart. The opening, called the ductus arteriosus, is a normal part of a baby's circulatory system before birth that usually closes shortly after birth. If it remains open, however, it's called a patent ductus arteriosus. A small patent ductus arteriosus often doesn't cause problems and might never need treatment. However, a large patent ductus arteriosus left untreated can allow poorly oxygenated blood to flow in the wrong direction, weakening the heart muscle and causing heart failure and other complications. Treatment options for a patent ductus arteriosus include monitoring, medications and closure by cardiac catheterization or surgery.
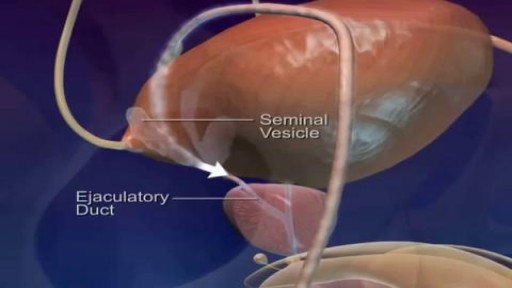
Watch that video of Pathway and Ejaculation of Sperm

Possible complications could include: Difficulty healing. Infection. Stump pain (severe pain in the remaining tissue) Phantom limb pain (a painful sensation that the foot or toe is still there) Continued spread of gangrene, requiring amputation of more areas of your foot, toes or leg. Bleeding. Nerve damage.

Traditional Liposuction VS Vaser Liposuction
A side-by-side comparison of traditional liposuction and a #Vaser liposuction. Both of these were performed by our skilled surgeons at Divine Cosmetic Surgery.
#vaserliposuction #liposuction #liposuctionDelhi #liposuctionresults #shorts #vaserliposuctionDelhi
Know more about liposuction
https://www.divinecosmeticsurg....ery.com/liposuction-
Traditional Liposuction vs 360 High Def Vaser Liposuction - https://www.youtube.com/watch?v=r_bBI2p9fVI&t=14s
-------------------------------------------------------------------------------
Why Vaser Is Best For Thigh Liposuction - https://youtu.be/dlzpdDEZcS4
-------------------------------------------------------------------------------
Abdomen Vaser Liposuction - Live - https://www.youtube.com/watch?v=_Cvl2Txn8LQ
-------------------------------------------------------------------------------
Back Vaser Liposuction In Female - https://youtu.be/OC60UdgtIWU
-------------------------------------------------------------------------------
For more details about Liposuction Visit - https://www.divinecosmeticsurgery.com/
-------------------------------------------------------------------------------
Dr. Amit Gupta
MBBS, M.S., DNB (Plastic & Cosmetic Surgery)
Divine Cosmetic Surgery | +91 9811994417
info@divinecosmeticsurgery.com | 01141828787
Delhi | Mumbai | Gurgaon
𝗦𝗼𝗰𝗶𝗮𝗹 𝗠𝗲𝗱𝗶𝗮 𝗮𝗻𝗱 𝗬𝗼𝘂𝘁𝘂𝗯𝗲 𝘃𝗶𝗱𝗲𝗼 𝗰𝗵𝗮𝗻𝗻𝗲𝗹 : -
🎦 https://www.youtube.com/c/DrAm....itGuptaBestPlasticCo
👍🏻 https://www.facebook.com/dramitguptaplasticsurgeon
📷 https://www.instagram.com/divineaesthetics_delhi/
🐥 https://twitter.com/dramitguptajee
🖇️ https://www.linkedin.com/compa....ny/divinecosmeticsur
📌 https://pinterest.com/divinesurgery
#Liposuction #vaserliposuction #liposuctioncostinindia #liposuctiondelhi #liposuction #liposuctioncost #liposuctioncostfactors #liposuctioncostindelhi #DrAmitGuptaPlasticSurgeon #DivineCosmeticSurgery #dramitgupta
Disclaimer: The information on our videos & social media is provided for informational purposes only and is not meant for the advice provided by your surgeon.
We are not responsible for any harm if anyone misguides you from our name. Our all-social media official handles are linked up on our website. All images & content used on our videos & social media are for illustrative concerns only, original results and processes may vary.

Getting Out of Bed after Surgery

In this episode of Crash Course Anatomy & Physiology, Hank gives you a brief history of histology and introduces you to the different types and functions of your body's tissues.
Pssst... we made flashcards to help you review the content in this episode! Find them on the free Crash Course App!
Download it here for Apple Devices: https://apple.co/3d4eyZo
Download it here for Android Devices: https://bit.ly/2SrDulJ
Chapters:
Introduction 00:00
Nervous, Muscle, Epithelial & Connective Tissues 1:23
History of Histology 2:07
Nervous Tissue Forms the Nervous System 5:17
Muscle Tissue Facilitates All Your Movements 7:00
Identifying Samples 9:03
Review 9:48
Credits 10:22
Crash Course is on Patreon! You can support us directly by signing up at http://www.patreon.com/crashcourse
Want to find Crash Course elsewhere on the internet?
Facebook - http://www.facebook.com/YouTubeCrashCourse
Twitter - http://www.twitter.com/TheCrashCourse
Instagram - https://www.instagram.com/thecrashcourse/
CC Kids: http://www.youtube.com/crashcoursekids

Eric's Home Dialysis

men health,women health,organ devloping ,female problems soultion,

fetal position in womb at 34 weeks fetal position in womb week by week fetal position in womb at 19 weeksUnborn babies toss and turn and hold many different positions within the womb during the gestation period; pregnant women everywhere will attest to the fact that their children always start up the gymnastics at bedtime.
